
Glasgow Coma Scale in Nursing Assessment: A Complete Guide to Interpretation and Clinical Application
The Glasgow Coma Scale is a foundational tool in neurological evaluation, offering a structured and objective way to assess a patient’s level of consciousness across a wide range of clinical situations. It is widely used in emergency care, critical care, and general clinical settings to evaluate patients with acute neurological impairment, including those with brain injury or altered mental status. Its continued relevance lies in its ability to provide a rapid, standardized measure of brain function that supports timely and appropriate clinical decision-making.
At its core, the Glasgow Coma Scale is built on a systematic assessment of three key components. These components allow clinicians to evaluate neurological status in a consistent and reproducible manner:
- Eye opening response
- Assesses arousal and awareness of the environment
- Ranges from spontaneous eye opening to no response
- Verbal response
- Evaluates the patient’s ability to communicate and orient
- Includes responses from fully oriented conversation to no verbal output
- Motor response
- Measures the patient’s ability to follow commands or respond to stimuli
- Ranges from purposeful movement to absence of motor activity
Each of these components is scored individually and then combined to form a total score. This structured scoring system enables healthcare providers to:
- Assess neurological status objectively rather than relying on subjective impressions
- Track changes over time, identifying early signs of deterioration or improvement
- Communicate findings clearly among members of the healthcare team
- Guide clinical interventions, particularly in acute and critical care scenarios
In clinical practice, the Glasgow Coma Scale plays a central role in patient monitoring and ongoing assessment. Nurses, in particular, are responsible for performing frequent neurological observations, making their ability to accurately assess and interpret findings essential. For example:
- A declining score over time may indicate increasing intracranial pressure or worsening brain injury
- A sudden change in response may signal acute complications such as hemorrhage or hypoxia
- Consistent scoring allows for early escalation of care and timely intervention
However, while the Glasgow Coma Scale is straightforward in structure, its application requires careful clinical judgment. Several factors can influence assessment findings, including:
- Sedation or analgesia
- Endotracheal intubation affecting verbal response
- Facial or orbital trauma limiting eye opening
- Underlying neurological disorders
These factors highlight the importance of not only performing the assessment correctly but also interpreting results within the broader clinical context.
This guide provides a comprehensive exploration of the Glasgow Coma Scale, focusing on its role in nursing assessment, its interpretation in different clinical scenarios, and its application in patient care. It examines the principles underlying the scoring system, outlines step-by-step assessment techniques, and discusses how the scale is used to guide treatment decisions and monitor neurological status. Through a detailed and structured approach, the discussion aims to deepen understanding of the Glasgow Coma Scale and support accurate, consistent, and clinically meaningful use in practice.
Behind on nursing research or documentation tasks?
We’ll complete your assignments with clarity and precision.
Foundations of the Glasgow Coma Scale in Nursing Assessment and Clinical Practice
Definition, Purpose, and Clinical Relevance of the Glasgow Coma Scale
The Glasgow Coma Scale is a standardized neurological assessment tool used to assess and quantify a patient’s level of consciousness. It provides a structured framework for evaluating brain function through observable responses, allowing clinicians to assign a gcs score that reflects the patient’s neurological status at a specific point in time.
At its most basic level, the Glasgow Coma Scale serves as both a definition of measurable consciousness and a practical method to evaluate patients across a spectrum of neurological conditions, from mild confusion to a comatose state. It is commonly used in emergency, trauma, and critical care clinical settings, particularly in patients with head injury, brain injury, or suspected traumatic brain injury.
The primary purpose of the Glasgow Coma Scale can be understood through its key clinical functions:
- Objective measurement
- Provides a numerical score to describe neurological status
- Reduces subjectivity in clinical evaluation
- Standardized communication
- Enables consistent reporting between nurses, physicians, and the healthcare team
- Facilitates rapid decision-making in acute situations
- Monitoring and trend analysis
- Supports ongoing monitoring of neurological status
- Detects early decrease in consciousness
- Clinical decision support
- Helps guide airway management (e.g., when to intubate)
- Assists in determining need for intervention or neurosurgical referral
Clinical example:
A patient presenting after a road traffic accident may initially appear alert but becomes less responsive over time. Repeated use of the Glasgow Coma Scale allows the nurse to detect subtle changes in motor response, verbal response, and eye opening. A declining number over successive assessments can indicate worsening intracranial pressure (ICP) or evolving hemorrhage, prompting urgent escalation of care.
Historical Development and Evolution of the Glasgow Coma Scale (Since 1974)
The Glasgow Coma Scale was first introduced in 1974 by neurosurgeons at the University of Glasgow as a method to simplify the examination of patients with acute brain injury. Prior to its development, clinicians relied on inconsistent and subjective descriptions of consciousness, making it difficult to compare patient status across providers or institutions.
The original GCS was designed to standardize neurological assessment by focusing on observable patient responses rather than complex neurological testing. Key goals included:
- Creating a widely used and reproducible scoring system
- Improving accuracy in assessing severity of injury
- Enabling clinicians to predict patient outcome more reliably
Over the past 50 years ago, the Glasgow Coma Scale has undergone refinements but remains fundamentally unchanged due to its simplicity and strong reliability. It is now a cornerstone in the assessment of traumatic brain injuries and is routinely used by:
- Nurses in bedside practice
- Emergency responders in prehospital care
- Physicians and surgeon teams in trauma units
Its continued use globally highlights its adaptability across diverse clinical settings, from high-resource intensive care units to resource-limited environments.
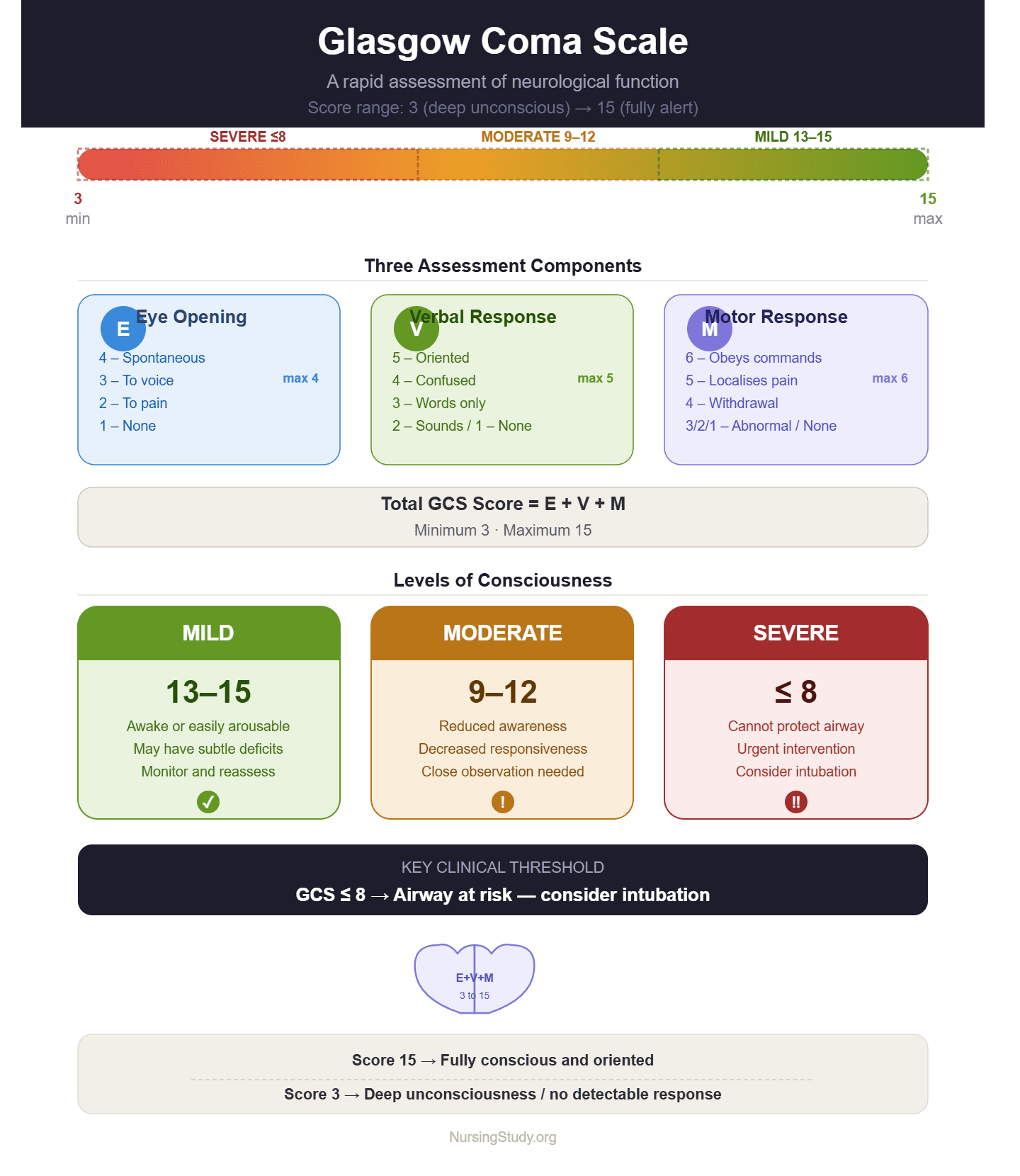
Understanding the Glasgow Coma Scale Scoring System (3–15) and Levels of Consciousness
The Glasgow Coma Scale assigns a score based on three components, each reflecting a different aspect of neurological function. The combined total produces a possible GCS range from 3 to 15, where:
- Score of 15 → Fully conscious and oriented
- Score of 3 → Deep unconsciousness or no detectable response
The three components include:
- Eye Opening (E)
- Verbal (V)
- Motor (M)
Each component is assessed individually, and their sum forms the total gcs score.
Levels of Consciousness Based on GCS
The total score provides a quick indicator of severity:
- Mild impairment (13–15)
- Patient is awake or easily arousable
- May still have subtle cognitive deficits
- Moderate impairment (9–12)
- Reduced awareness and responsiveness
- Requires close observation and monitoring
- Severe impairment (≤8)
- Often associated with inability to protect airway
- A score of 8 or less may indicate need to intubate
Key Clinical Considerations
- Lower GCS scores are associated with increased risk of complications and poorer outcome
- The scale is particularly valuable in tbi and other acute neurological emergencies
- Repeated assessment is more important than a single measurement
Example:
A patient with a gcs score of 8 following a head injury may exhibit abnormal motor posturing and incomprehensible verbal response. This finding signals a severe neurological impairment and requires immediate airway protection and further clinical evaluation.
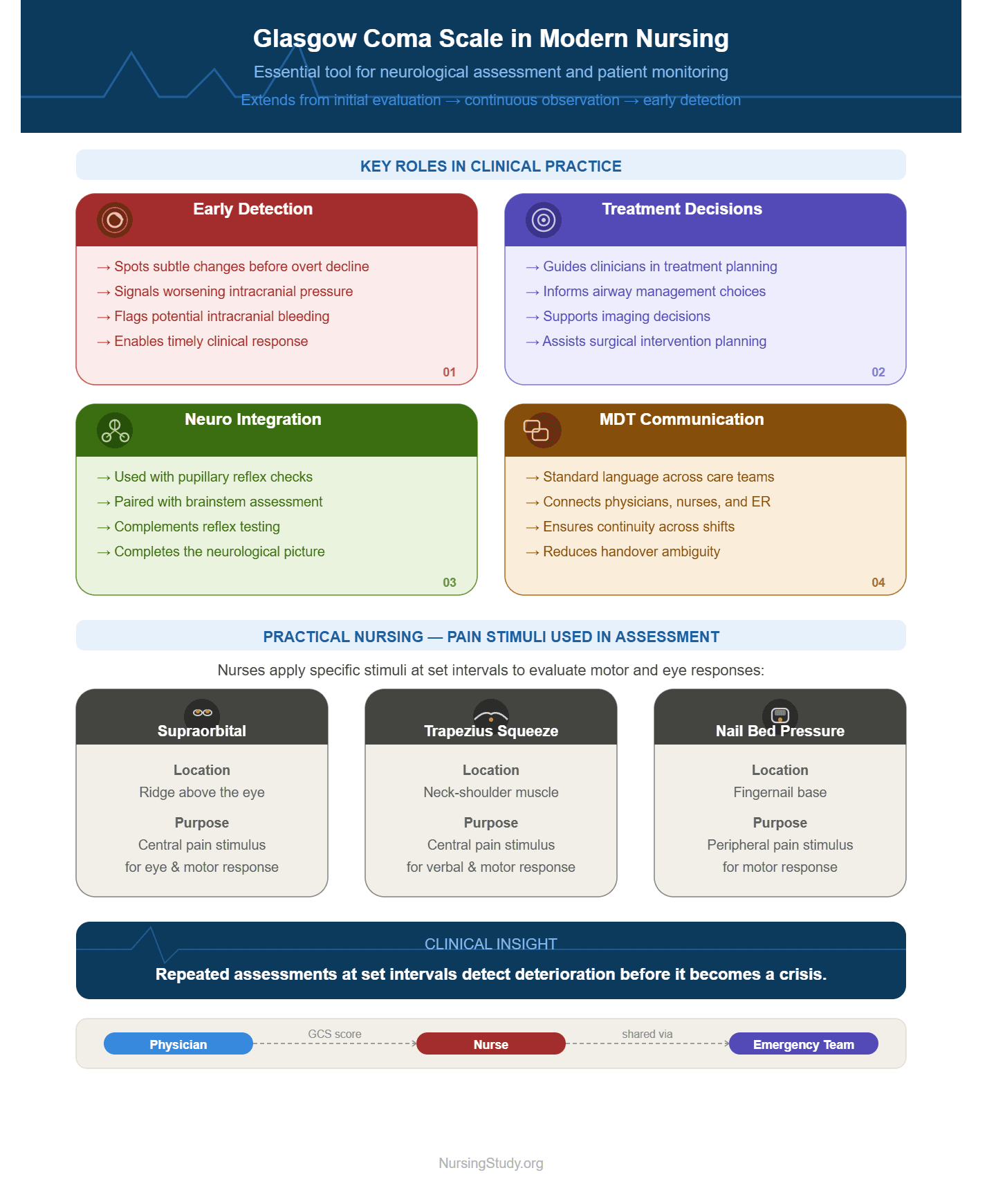
Importance of the Glasgow Coma Scale in Modern Nursing and Neurological Assessment
In modern nursing practice, the Glasgow Coma Scale is an essential component of neurological assessment and patient monitoring. Its role extends beyond initial evaluation to continuous observation and early detection of deterioration.
Key Roles in Clinical Practice
- Early detection of deterioration
- Identifies subtle changes before overt clinical decline
- Acts as an indicator of worsening intracranial pressure or bleeding
- Guiding treatment decisions
- Helps clinicians guide treatment plans
- Supports decisions regarding airway, imaging, and surgical intervention
- Integration with neurological examination
- Used alongside pupillary checks, reflex testing, and brainstem assessment
- Provides a more complete neurological picture
- Supporting multidisciplinary communication
- Enables clear reporting between the physician, nurse, and emergency team
- Ensures continuity of care across shifts
Practical Nursing Application
Nurses frequently perform repeated Glasgow Coma Scale examination at set intervals. During these assessments, they may use specific stimuli to evaluate responses, including:
- Supraorbital pressure
- Trapezius muscle squeeze
- Nail bed pressure on the nail
These stimuli help determine the best motor response and overall neurological status.
Clinical scenario:
A patient admitted with traumatic brain injury initially presents with a moderate score. Over several hours, the nurse notes a gradual decrease in responsiveness and worsening motor response. This change serves as a critical warning sign of rising ICP, prompting urgent imaging and possible neurosurgical intervention.
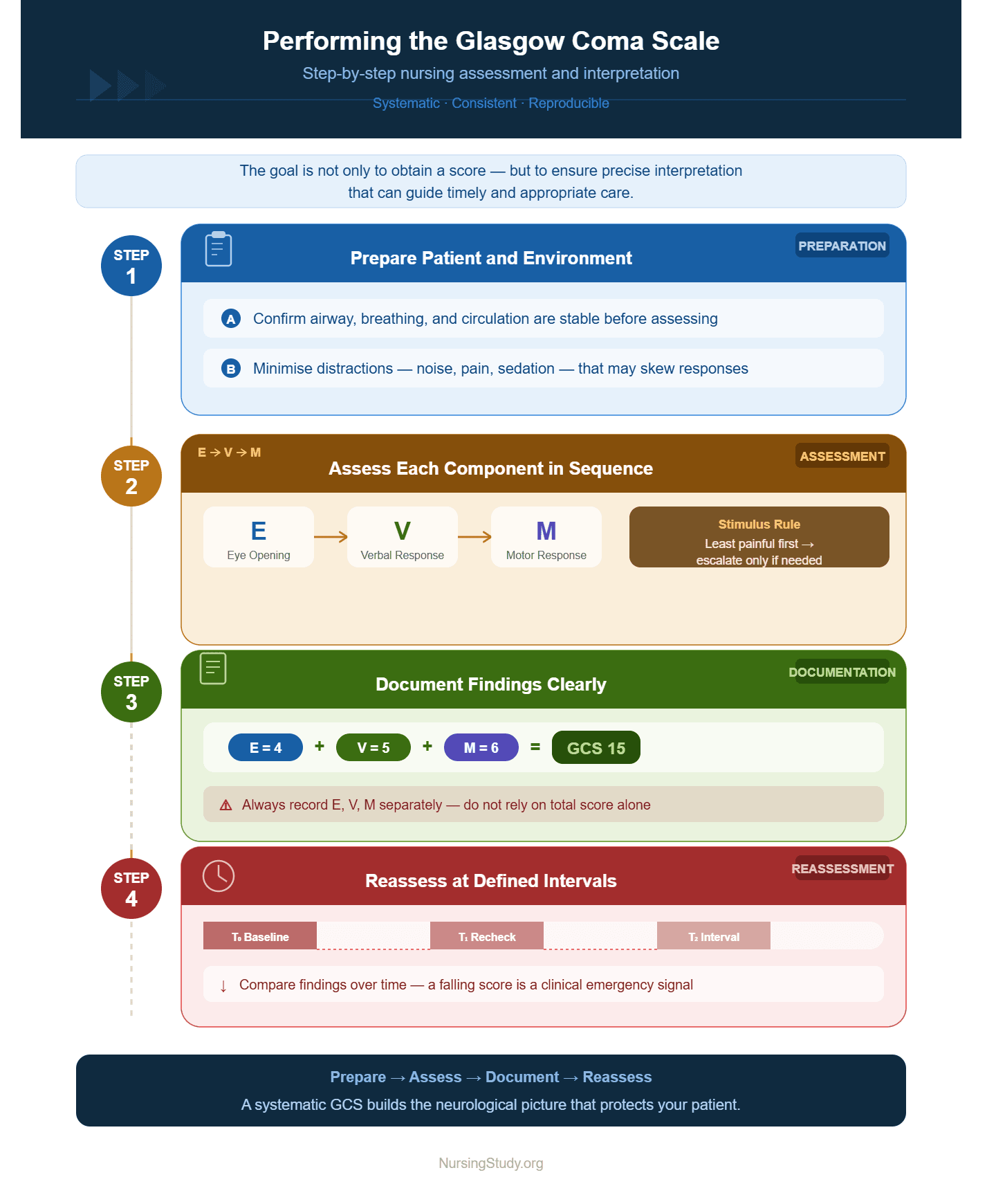
Performing the Glasgow Coma Scale: Step-by-Step Nursing Assessment and Interpretation
Accurate performance of the Glasgow Coma Scale requires a systematic, consistent, and reproducible approach. In clinical practice, each component must be evaluated carefully using appropriate stimulus, ensuring that responses reflect true neurological status rather than external influences. The goal is not only to obtain a score, but to ensure precise interpretation that can guide timely and appropriate care.
A structured approach to performing the Glasgow Coma Scale includes:
- Prepare the patient and environment
- Ensure airway, breathing, and circulation are stable
- Minimize distractions that may affect responses
- Assess each component in sequence
- Eye opening → Verbal → Motor
- Use the least painful stimulus first, escalating only if necessary
- Document findings clearly
- Record each component separately (E, V, M)
- Avoid relying on total score alone
- Reassess at defined intervals
- Compare findings over time to detect deterioration
Eye Opening Response: Assessment Technique and Clinical Interpretation
Eye opening reflects arousal mechanisms controlled by higher cortical centers and the brainstem. It is often the first observable indicator of a patient’s level of consciousness.
Assessment Technique
Eye opening is assessed in a stepwise manner:
- Spontaneous: Patient opens eyes without prompting
- To voice: Opens eyes when spoken to
- To pain: Opens eyes only after application of painful stimulus
- No response: No eye opening at all
When pain is required, commonly used techniques include:
- Supraorbital pressure
- Trapezius muscle squeeze
These methods ensure that the response reflects central neurological processing rather than peripheral reflexes.
Clinical Interpretation
- Spontaneous eye opening suggests intact arousal pathways
- Eye opening only to pain indicates reduced cortical activity
- Absence of response may indicate severe dysfunction or progression toward a comatose state
Example:
A patient who initially opens eyes to voice but later requires painful stimulus demonstrates a decline in neurological status, which may indicate worsening intracranial pressure or evolving hemorrhage.
Verbal Response: Evaluation, Scoring, and Interpretation in Clinical Settings
The verbal component assesses cognitive function, orientation, and ability to communicate. It reflects both cortical processing and integration of sensory input.
Evaluation Approach
The patient is asked simple questions to determine orientation:
- Name
- Location
- Time
Responses are categorized as:
- Oriented: Fully aware and coherent
- Confused: Disoriented but able to respond
- Inappropriate words: Random or irrelevant speech
- Incomprehensible sounds: Moaning or groaning
- No response
Clinical Considerations
- Patients who are intubated cannot provide verbal responses
- In such cases, documentation should reflect limitation rather than assigning a misleading low score
Interpretation
- An oriented response suggests intact higher brain function
- Confusion may indicate early neurological compromise
- Incomprehensible or absent responses often reflect severe impairment
Example:
A patient with a head injury who becomes progressively confused may be developing complications such as swelling or bleeding, requiring urgent reassessment.
Motor Response: Assessing Best Motor Response and Clinical Significance
The motor response is the most reliable component of the Glasgow Coma Scale and a key predictor of neurological outcome. It evaluates the patient’s ability to respond purposefully to commands or painful stimuli.
Assessment Steps
- Give a simple command
- Ask the patient to move a limb
- If no response, apply pain
- Use central stimuli such as trapezius squeeze
- Observe the best response
- Record the highest level of movement observed
Categories of Motor Response
- Obeys commands
- Localizes pain
- Withdraws from pain
- Abnormal flexion (decorticate)
- Abnormal extension (decerebrate)
- No response
Clinical Interpretation
- Purposeful movement indicates preserved cortical function
- Abnormal posturing suggests significant neurological damage
- No response is associated with severe brain dysfunction
Example:
A patient who initially withdraws from pain but later demonstrates abnormal extension is showing signs of worsening severity, often linked to increasing intracranial pressure (ICP) or brain herniation risk.
Calculating the Total Glasgow Coma Scale Score and Ensuring Accuracy
After assessing each component, scores are combined to produce the total Glasgow Coma Scale score. This total provides a quick summary of neurological status but must always be interpreted alongside individual component findings.
Calculation
- Eye opening (E) + Verbal (V) + Motor (M) = Total score
- Range: lowest possible score to highest possible score
Ensuring Accuracy
To maintain accuracy and reliability, the following principles should be applied:
- Score components individually rather than estimating
- Avoid assumptions when responses are limited (e.g., intubation)
- Use consistent techniques for applying stimulus
- Document clearly in the chart
Common Pitfalls
- Misinterpreting reflex movements as purposeful
- Failing to reassess after interventions
- Over-reliance on total score without clinical context
Clinical Application
- A declining score over time is a critical indicator of deterioration
- Stable scores suggest neurological stability
- Improvement may indicate effective treatment
Example:
A patient with traumatic brain injury may initially have a moderate score. With proper management, including airway support and monitoring, the score may improve, reflecting recovery of brain function. Conversely, a decrease in score signals need for urgent reassessment and possible intervention.
Clinical Interpretation of Glasgow Coma Scale Scores in Neurological Conditions
Clinical interpretation of the Glasgow Coma Scale focuses on translating a numerical score into meaningful information about a patient’s neurological status. In practice, the gcs score reflects the severity of brain dysfunction and helps guide urgent decisions in patients with altered consciousness due to neurological conditions such as traumatic brain injury, head injury, stroke, or intracranial bleeding.
Rather than viewing the score in isolation, clinicians interpret it alongside clinical findings such as pupillary reaction, respiratory pattern, and hemodynamic stability. This integrated approach ensures that the level of consciousness is accurately understood in real-world clinical contexts.
Classification of Glasgow Coma Scale Scores: Mild, Moderate, and Severe Impairment
The Glasgow Coma Scale divides neurological impairment into clinically meaningful categories based on the total score. This classification helps standardize communication and guides urgency of care.
1. Mild impairment (13–15)
Patients in this range are generally conscious and responsive, though they may still have subtle neurological deficits.
- Usually alert or easily arousable
- May show mild confusion or disorientation
- Often able to follow commands
Clinical example:
A patient after a minor head injury may present with a score of 14 due to temporary confusion but remains responsive and stable under observation.
2. Moderate impairment (9–12)
This range indicates a significant reduction in neurological function.
- Reduced awareness of surroundings
- Inconsistent responses to verbal commands
- May require close monitoring for deterioration
Clinical example:
A patient with a traumatic brain injury who opens eyes only to voice and produces confused speech may fall into this category, requiring frequent reassessment for possible worsening brain injury or rising intracranial pressure.
3. Severe impairment (3–8)
This range indicates critical neurological compromise and often correlates with coma.
- Minimal or no response to stimuli
- Abnormal motor posturing or no motor activity
- High risk of airway compromise
Clinical importance:
A score of 8 or less is widely recognized as a threshold for considering airway protection through intubation, due to loss of protective reflexes and risk of respiratory failure.
Interpreting the Glasgow Coma Scale in Traumatic Brain Injury and Head Injury
In cases of traumatic brain injury (TBI) and head injury, the Glasgow Coma Scale is one of the most important tools for assessing injury severity and tracking progression.
The scale helps clinicians:
- Determine initial injury severity
- Monitor changes in neurological status over time
- Identify early signs of deterioration
Clinical interpretation in TBI
- A declining score often indicates worsening cerebral edema, hemorrhage, or hypoxia
- A stable score suggests neurological stability under current management
- Improvement may indicate recovery or effective intervention
Example:
A patient admitted after a motor vehicle accident initially has a score of 13. Over several hours, the score drops to 10 with worsening motor response. This change may suggest expanding intracranial bleeding, requiring urgent imaging and neurosurgical evaluation.
Clinical Significance of Low Glasgow Coma Scale Scores and Critical Decision-Making
Low Glasgow Coma Scale scores carry significant clinical implications and often require immediate intervention. A score of 8 or less is particularly critical and is associated with severe neurological dysfunction.
Clinical significance includes:
- Loss of airway protection reflexes
- Increased risk of aspiration and respiratory failure
- Possible elevation in intracranial pressure (ICP)
- Need for urgent critical care management
Key decision-making considerations
- Airway management: Patients with low scores may require intubation
- Neurological escalation: Immediate referral to neurosurgical teams may be necessary
- Advanced monitoring: Continuous ICU-level observation is often required
Clinical example:
A patient with a severe head injury presents with a score of 7, absent verbal response, and abnormal extension to pain. This presentation signals a high-risk neurological emergency requiring rapid airway stabilization and urgent imaging to rule out hemorrhage.
Prognostic Value of the Glasgow Coma Scale in Patient Outcomes
The Glasgow Coma Scale is widely used as a prognostic indicator in patients with acute brain injury and other neurological emergencies. It helps estimate likely outcomes, including recovery potential, disability, and mortality risk.
Prognostic applications include:
- Mortality prediction: Lower scores are associated with higher risk of death
- Functional outcome estimation: Helps anticipate long-term disability or recovery
- Treatment planning: Guides intensity of care and resource allocation
Relationship between score and outcome
- Higher scores (13–15): Generally favorable outcomes
- Moderate scores (9–12): Variable outcomes depending on cause and intervention
- Low scores (3–8): Increased risk of poor outcome or mortality
Clinical example
A patient with a score of 5 following a severe traumatic brain injury has a significantly higher risk of mortality compared to a patient with a score of 14 following a mild head injury. This difference influences decisions regarding intensive care admission, surgical intervention, and family counseling.
Limitations and Clinical Challenges in Glasgow Coma Scale Interpretation
Although the Glasgow Coma Scale is widely used in neurological assessment and critical care, its application is not without limitations. In real-world clinical settings, interpretation of the gcs score can be influenced by multiple physiological, environmental, and procedural factors that may affect its accuracy and reliability. Understanding these limitations is essential for ensuring safe clinical decision-making, especially in patients with traumatic brain injury, head injury, or other acute neurological conditions.
A key challenge is that the Glasgow Coma Scale measures observable responses rather than direct brain function, meaning it can be influenced by conditions that do not reflect true neurological status. As a result, clinicians must interpret findings within a broader clinical context rather than relying solely on the numerical score.
Factors Affecting Accuracy in Glasgow Coma Scale Assessment
Several factors can significantly influence the accuracy of Glasgow Coma Scale assessment, potentially leading to misinterpretation of a patient’s level of consciousness. These factors must always be considered during examination and documentation.
1. Medical and physiological factors
- Sedation and anesthesia: Patients receiving sedatives may appear less responsive, artificially lowering the score
- Alcohol or drug intoxication: Can suppress neurological responses without structural brain damage
- Hypoxia or hypoglycemia: May temporarily reduce responsiveness, mimicking brain injury
- Cardiac arrest or shock states: Reduced cerebral perfusion affects responsiveness
2. Neurological and structural factors
- Severe brain injury or hemorrhage: True reduction in responsiveness due to structural damage
- Increased intracranial pressure (ICP): Can cause progressive neurological decline
- Brainstem dysfunction: Directly affects arousal and reflex responses
3. Physical and trauma-related limitations
- Facial trauma or swelling: May prevent proper eye opening assessment
- Spinal or limb injuries: Can limit motor response evaluation
- Use of paralytics: Completely suppresses motor activity
4. Clinical procedure-related limitations
- Intubation: Prevents accurate assessment of verbal response
- Tracheostomy or airway devices: Alters verbal scoring interpretation
Clinical example:
A patient in intensive care who is sedated and mechanically ventilated after neurosurgical intervention may have a low gcs score of 8 or less, but this does not necessarily reflect worsening neurological status. Instead, it reflects pharmacological suppression of responsiveness.
When the Glasgow Coma Scale Is Insufficient in Clinical Evaluation
While the Glasgow Coma Scale is an essential tool, there are clinical situations where it is insufficient as a standalone measure of neurological status. This is particularly true when deeper insight into brainstem or cortical function is required.
Situations where the scale is limited
- Intubated or mechanically ventilated patients
- Verbal response cannot be assessed, limiting full scoring
- Severe facial or cranial trauma
- Eye opening and verbal components may be unreliable
- Neuromuscular blockade use
- Motor response is absent despite preserved brain function
- Complex neurological disorders
- Conditions such as locked-in syndrome may produce misleading scores
Need for complementary assessment
In these cases, clinicians rely on additional neurological evaluation methods such as:
- Pupillary response testing
- Brainstem reflexes
- Respiratory pattern assessment
- Advanced neuroimaging and monitoring tools
Clinical example:
A patient with locked-in syndrome may have near-normal consciousness but appears unresponsive due to paralysis. In such cases, the Glasgow Coma Scale alone would incorrectly suggest severe impairment, highlighting its limitations in certain neurological conditions.
Inter-Observer Variability and Improving Reliability in Nursing Assessment
Another major challenge in Glasgow Coma Scale interpretation is inter-observer variability, where different healthcare providers assign different scores to the same patient. This can significantly affect communication, treatment decisions, and continuity of care.
Causes of variability
- Differences in clinical experience among healthcare professionals
- Inconsistent application of assessment techniques
- Misinterpretation of subtle motor or verbal responses
- Variation in stimulus application (e.g., pressure intensity on trapezius or nail bed)
- Lack of standardized training or refresher education
Impact on clinical practice
- Inconsistent documentation in patient records
- Delayed recognition of neurological deterioration
- Miscommunication between nursing and medical teams
- Potential delays in intervention for worsening conditions such as intracranial hemorrhage
Strategies to improve reliability
To enhance consistency and improve reliability, clinical teams should adopt structured approaches:
- Standardized training programs
- Regular competency assessments for staff performing neurological evaluation
- Clear documentation practices
- Recording individual components (E, V, M) rather than only total score
- Use of consistent stimulus methods
- Standardizing techniques such as trapezius squeeze or supraorbital pressure
- Frequent reassessment and comparison
- Monitoring trends over time rather than relying on single measurements
- Team communication protocols
- Ensuring consistent interpretation across nurses, physicians, and emergency staff
Clinical example:
Two nurses assessing the same patient with a traumatic brain injury may initially assign slightly different scores due to variation in interpreting motor withdrawal. Through standardized training and structured assessment tools, these discrepancies can be minimized, improving patient safety and clinical decision-making.
Nursing Application: Charting, Monitoring, and Clinical Decision-Making Using the Glasgow Coma Scale
In clinical practice, the Glasgow Coma Scale is not only an assessment tool but also a critical component of ongoing patient management. It plays a central role in monitoring neurological status, guiding clinical decisions, and supporting timely escalation of care in patients with traumatic brain injury, head injury, stroke, and other acute neurological conditions.
For nursing practice, the value of the Glasgow Coma Scale extends beyond obtaining a single gcs score—it lies in trend observation, accurate documentation, and integration with broader neurological evaluation.
Accurate Documentation and Charting of Glasgow Coma Scale Scores
Precise charting of the Glasgow Coma Scale is essential for ensuring continuity of care and effective communication among healthcare teams. Inaccurate or incomplete documentation can lead to misinterpretation of a patient’s condition and delay critical interventions.
Key principles of accurate documentation
When recording a Glasgow Coma Scale assessment, the following must be included:
- Individual component scores (E + V + M) rather than only total score
- Total score clearly documented (e.g., E3 V4 M6 = 13)
- Time of assessment to allow comparison over intervals
- Patient condition influencing score, such as sedation or intubation
- Any changes in responsiveness or level of consciousness
Importance in clinical communication
Accurate charting ensures that:
- Physicians and nurses can assess changes quickly
- Trends in neurological status are clearly visible
- Decisions regarding escalation, imaging, or neurosurgical referral are supported
Clinical example
A patient admitted with traumatic brain injury may initially have a score of 14. If the score drops to 11 over several hours, clear documentation allows the next clinician to immediately recognize deterioration and initiate urgent evaluation for possible intracranial pressure (ICP) rise or hemorrhage.
Monitoring Trends and Recognizing Early Neurological Deterioration
One of the most important clinical uses of the Glasgow Coma Scale is monitoring changes over time rather than relying on a single measurement. Subtle changes in motor response, verbal response, or eye opening may indicate early neurological decline.
Why trend monitoring is essential
- The brain can deteriorate rapidly in conditions such as acute head injury or bleeding
- Early changes often appear before vital signs become abnormal
- Serial assessments help identify worsening brain function
Key warning signs of deterioration
- Progressive decrease in GCS score
- Loss of verbal responsiveness
- Declining motor response (e.g., withdrawal → abnormal posturing)
- Reduced responsiveness to painful stimulus
- New onset of pupillary asymmetry or sluggish reaction
Clinical significance
A drop of even 1–2 points in the Glasgow Coma Scale can be clinically significant, especially in moderate or severe injury cases.
Clinical example
A patient with a stable score of 13 following a fall becomes increasingly drowsy, eventually scoring 10. This change in score may suggest expanding intracranial bleeding, requiring immediate imaging and possible surgical intervention.
Integrating the Glasgow Coma Scale with Other Clinical Assessment Tools
Although the Glasgow Coma Scale is a powerful tool, it is most effective when combined with other neurological and physiological assessments. This integrated approach provides a more complete picture of the patient’s condition.
Key complementary assessment tools
- Pupillary assessment
- Evaluates size, symmetry, and reaction to light
- Helps detect brainstem dysfunction
- Brainstem reflexes
- Includes corneal reflex and gag reflex
- Provides deeper insight into neurological integrity
- Respiratory assessment
- Abnormal breathing patterns may indicate brain injury progression
- Helps assess respiratory drive in severe cases
- Hemodynamic monitoring
- Blood pressure and heart rate changes may reflect raised ICP or shock
- Imaging and diagnostic tools
- CT or MRI scans confirm structural damage such as hemorrhage or swelling
Why integration is essential
- The Glasgow Coma Scale alone cannot detect all aspects of neurological injury
- Combined assessment improves diagnostic accuracy
- Supports early identification of life-threatening conditions
Clinical example
A patient with a GCS score of 9 after a traumatic brain injury also shows unequal pupils and irregular breathing patterns. While the score alone indicates moderate impairment, integration with pupillary and respiratory findings suggests possible brainstem involvement, prompting urgent neurosurgical evaluation.
Behind on nursing research or documentation tasks?
We’ll complete your assignments with clarity and precision.
Conclusion
The Glasgow Coma Scale remains one of the most essential tools in neurological assessment, providing a structured and standardized method for evaluating level of consciousness across a wide range of clinical settings. Its strength lies in its simplicity—translating complex brain activity into a measurable gcs score based on eye opening, verbal response, and motor response. This structured approach allows clinicians to rapidly assess patients with traumatic brain injury, head injury, stroke, and other acute neurological conditions, supporting timely recognition of deterioration and appropriate intervention.
Across all stages of care, the Glasgow Coma Scale plays a critical role in guiding clinical decision-making, particularly in emergency and critical care environments. A falling score may signal worsening brain function, rising intracranial pressure, or evolving neurological compromise, while stable or improving scores may indicate recovery. However, its true value is only realized when it is applied consistently, interpreted in context, and integrated with other assessments such as pupillary responses, reflex testing, and physiological monitoring.
Despite its widespread use, the scale is not without limitations. Factors such as sedation, intubation, and coexisting medical conditions can affect accuracy, highlighting the importance of clinical judgment alongside numerical scoring. Additionally, variations in interpretation emphasize the need for standardized training and consistent practice to improve reliability in nursing assessment.
Ultimately, the Glasgow Coma Scale is more than a scoring system—it is a dynamic clinical tool that supports continuous monitoring, enhances communication among healthcare professionals, and strengthens the ability to respond promptly to neurological changes. When used correctly and thoughtfully, it contributes significantly to improved patient safety, more informed treatment decisions, and better outcomes in individuals experiencing acute neurological injury or illness.
Frequently Asked Questions
What is a normal Glasgow Coma Scale?
A normal score on the Glasgow Coma Scale is 15/15, which indicates that the patient is fully conscious, alert, and oriented with intact level of consciousness. A score of 15 reflects normal brain function, appropriate motor response, clear verbal response, and spontaneous eye opening.
How do you calculate the Glasgow Coma Score?
The Glasgow Coma Score is calculated by adding the scores from three separate assessments:
- Eye opening response
- Verbal response
- Motor response
Each component is assessed individually, and the final gcs score is the sum of all three. The total ranges from 3 to 15, where 3 indicates deep unconsciousness and 15 indicates full consciousness.
What are the three components of the Glasgow Coma Scale?
The Glasgow Coma Scale consists of three key components:
- Eye opening response (E)
- Verbal response (V)
- Motor response (M)
These components are used together to evaluate a patient’s neurological status and determine their overall level of consciousness.
What is the Glasgow Coma Scale assessment?
The Glasgow Coma Scale assessment is a structured neurological assessment used to evaluate and measure a patient’s level of consciousness following head injury, brain injury, or other neurological conditions. It involves observing and scoring eye opening, verbal communication, and motor responses to determine the patient’s gcs score, which helps guide clinical decision-making and ongoing monitoring.