
Wound Dehiscence vs Evisceration: A Comprehensive Guide to Abdominal Wound Dehiscence and Evisceration, Risk Factors, and Postoperative Wound Complications
Postoperative recovery following abdominal surgery is fundamentally dependent on the integrity of the surgical wound and the efficiency of the body’s wound healing process. Under normal conditions, a surgical incision progresses through predictable phases of healing, allowing the skin and muscle layers to regain strength and continuity. However, when this healing process is disrupted, significant wound complications may arise—most notably wound dehiscence and evisceration, which represent critical forms of surgical complication associated with increased morbidity and, in severe cases, a higher mortality rate.
At a foundational level, wound dehiscence refers to the separation of wound edges after initial wound closure, while evisceration represents a more advanced and severe progression in which the surgical incision reopens, allowing internal organs, particularly abdominal organs, to protrude through the open wound. These two conditions are closely related, with surgical wound dehiscence often acting as a precursor that may lead to evisceration if not promptly recognized and managed. When this occurs, the situation becomes a medical emergency that requires immediate medical and surgical intervention.
The occurrence of dehiscence and evisceration is rarely due to a single cause. Instead, it is typically the result of multiple interacting risk factors that impair the stability of the abdominal wall and compromise the integrity of the incision site. These factors can be broadly understood as follows:
- Patient-Related Risk Factors
- Obesity, which increases tension on the surgical wound and elevates intra-abdominal pressure
- Malnutrition, which impairs the body’s healing capacity and delays granulation
- Poorly controlled blood glucose, contributing to delayed healing and increased risk of infection
- Surgical and Technique-Related Factors
- Inadequate surgical technique or improper suture selection
- Excessive tension on the edges of the wound during wound closure
- Weakness in deeper structures such as the fascia, which plays a key role in maintaining abdominal integrity
- Postoperative and Environmental Factors
- Increased intra-abdominal pressure due to cough, sneeze, or heavy lifting
- Development of wound infection, which weakens tissue and contributes to wound breakdown
- Inadequate wound care, including poor dressing abdominal wound practices or failure to maintain a sterile environment
When these factors converge, they can result in a dehisced wound, where the wound edges begin to separate. Clinically, this may present with wound dehiscence symptoms such as:
- Sudden drainage from the surgical site
- Visible separation of wound layers
- A reported “popping” sensation as the wound reopens
- Signs of poor wound healing, including redness, swelling, or discharge
If not addressed promptly, this wound breakdown can progress to complete dehiscence, and in more severe cases, culminate in evisceration, where abdominal organs are exposed. This progression significantly increases the complexity of management, often necessitating urgent surgical intervention, prolonged hospitalization in a medical center, and advanced treatment options such as negative pressure wound therapy or delayed closure by secondary intention.
From a clinical perspective, the implications of wound dehiscence and evisceration extend beyond the immediate postoperative wound. These conditions can:
- Increase the likelihood of long-term complications such as hernia formation, requiring hernia repair
- Prolong the healing process, delaying recovery after abdominal procedures
- Elevate the overall risk of wound failure in future surgeries
Effective management begins with early recognition and appropriate intervention. Key immediate priorities include:
- Protecting the open wound and preventing contamination (e.g., cover the wound with a sterile dressing)
- Reducing strain on the abdominal wall, often using an abdominal binder
- Prompt communication with healthcare providers to initiate definitive care
Equally important is the role of preventing wound dehiscence through evidence-based strategies that support the body’s healing. These include optimizing nutrition, ensuring proper wound care, minimizing strain on the surgical incision, and maintaining strict infection control practices.
This discussion provides a comprehensive foundation for understanding wound dehiscence and evisceration as critical postoperative complications. By examining how these conditions develop, the factors that contribute to their occurrence, and their clinical implications, a clearer framework emerges for recognizing early warning signs, implementing timely interventions, and ultimately improving outcomes in patients undergoing abdominopelvic surgeries.
Introduction to Postoperative Wound Dehiscence and Evisceration as Surgical Complications
Postoperative recovery following abdominal surgery depends on the integrity of the surgical wound and the effectiveness of the body’s wound healing mechanisms. Under normal conditions, a surgical incision heals through a coordinated biological process that restores the continuity of the skin and muscle, strengthens the abdominal wall, and protects underlying internal organs. However, when this process is disrupted, patients may develop serious wound complications, most notably wound dehiscence and evisceration.
These complications exist along a clinical spectrum:
- Wound dehiscence involves the separation of wound edges, which may be superficial dehiscence (affecting skin layers) or complete dehiscence (involving deeper structures such as the fascia).
- Evisceration represents a severe progression where the surgical incision reopens, allowing abdominal organs to protrude through the open wound.
When dehiscence occurs, it compromises the structural integrity of the postoperative wound. If not recognized early, this breakdown can lead to evisceration, transforming a localized surgical complication into a life-threatening medical emergency that requires immediate medical and surgical intervention.
Why These Complications Occur
The development of wound dehiscence and evisceration is multifactorial and often linked to a combination of:
- Mechanical stress on the incision site
- Increased intra-abdominal pressure from activities such as cough, sneeze, or heavy lifting
- Excess tension across the edges of the wound due to poor surgical technique or tight suture placement
- Impaired healing conditions
- Poor wound healing caused by malnutrition, uncontrolled blood glucose, or reduced tissue perfusion
- Disruption of the body’s healing phases, including inflammation and granulation
- Infectious processes
- Wound infection, which weakens tissue and contributes to wound breakdown
- Increased risk of infection due to inadequate wound care or non-sterile conditions
- Structural weakness
- Failure of deep supporting layers such as the fascia
- Presence of broken sutures, leading to a dehisced wound
Clinical Progression
The transition from surgical wound dehiscence to evisceration typically follows a recognizable pattern:
- Early stage: subtle wound dehiscence symptoms such as redness, swelling, or serosanguinous drainage
- Intermediate stage: visible separation of wound edges and wound reopens partially (partial dehiscence)
- Advanced stage: complete wound dehiscence, exposing deeper layers
- Critical stage: evisceration, where abdominal organs become visible outside the surgical site
This progression highlights why early identification of a dehisced wound is essential to prevent escalation into severe cases.
Struggling with complex nursing topics?
We’ll simplify them into clear, concise, and professional assignments.
Overview of Postoperative Wound Healing in Abdominal Surgery
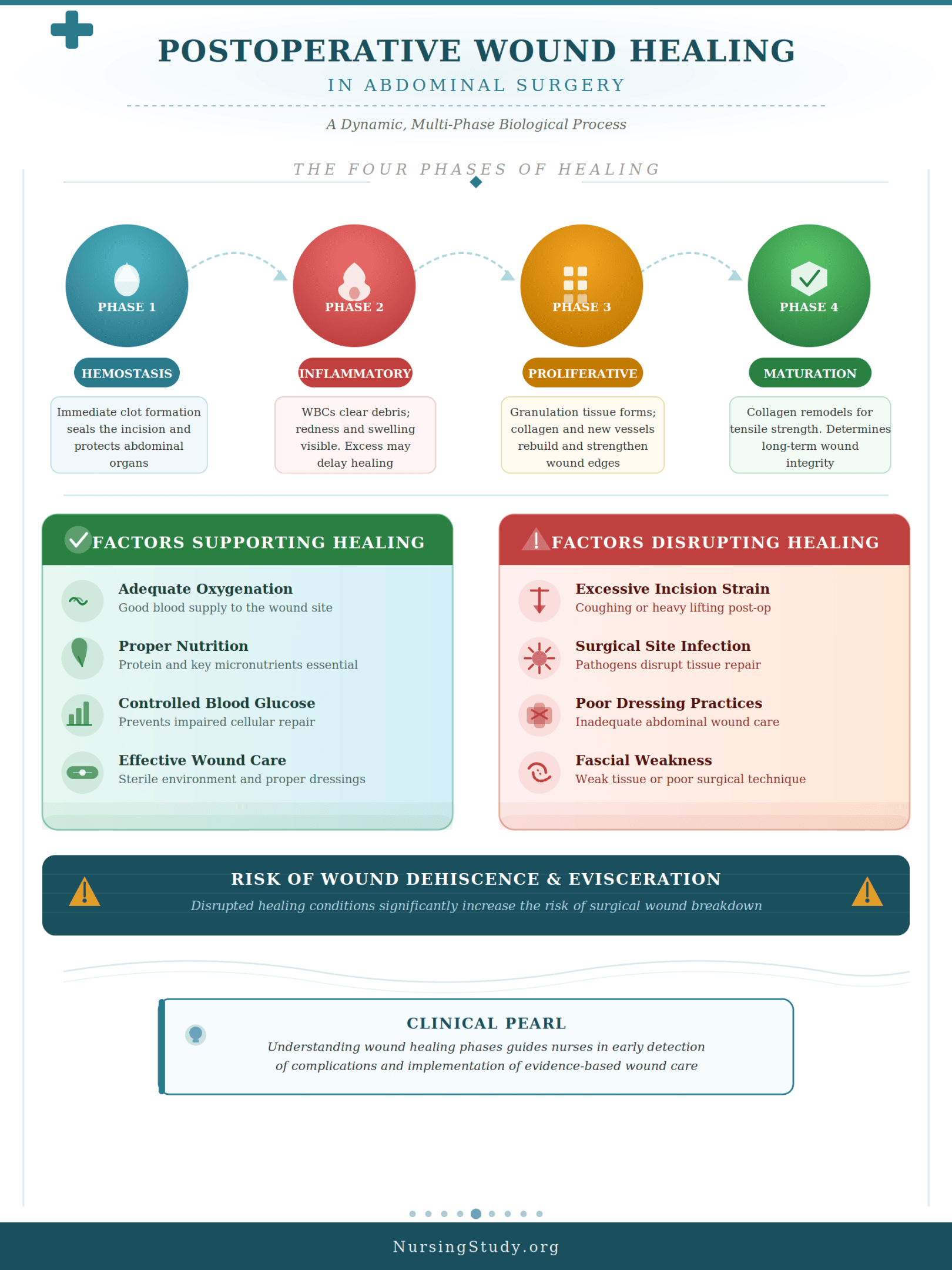
To understand wound dehiscence and evisceration, it is essential to first examine normal wound healing following abdominal procedures. The healing of a surgical incision is a dynamic and highly regulated process involving multiple overlapping phases:
1. Hemostasis Phase (Immediate Response)
- Occurs immediately after wound closure
- Blood clot formation stabilizes the incision site
- Provides a temporary barrier to protect underlying abdominal organs
2. Inflammatory Phase
- Characterized by localized swelling, redness, and immune activity
- White blood cells remove debris and prevent wound infection
- Excessive inflammation may contribute to delayed healing
3. Proliferative Phase
- Formation of granulation tissue
- Rebuilding of collagen and new blood vessels
- Gradual strengthening of the edges of the wound
4. Maturation (Remodeling) Phase
- Long-term strengthening of the abdominal wall
- Collagen fibers reorganize to improve tensile strength
- This phase determines whether the wound will close the wound effectively or remain vulnerable
Factors That Support Effective Healing
Successful wound healing depends on:
- Adequate oxygenation and blood supply
- Proper nutrition (protein and micronutrients)
- Controlled blood glucose levels
- Effective wound care and maintenance of a sterile environment
Factors That Disrupt Healing
When these conditions are compromised, the risk of dehiscence increases. Contributing factors include:
- Excessive strain on the surgical incision (e.g., cough, heavy lifting)
- Infection at the surgical site
- Poor dressing abdominal wound practices
- Weakness in the fascia or improper surgical technique
For example, a patient recovering from abdominopelvic surgeries who experiences persistent coughing may place repeated stress on the incision site, leading to gradual wound breakdown and eventual surgical wound dehiscence.
Clinical Significance of Wound Dehiscence and Evisceration in Nursing Practice
The occurrence of wound dehiscence and evisceration carries significant implications for patient safety, recovery outcomes, and healthcare delivery. These complications are not only physically debilitating but also associated with increased hospital stays, higher treatment costs, and elevated mortality rate in severe cases.
1. Impact on Patient Outcomes
- Increased risk of secondary complications such as hernia, often requiring hernia repair
- Prolonged healing process and delayed recovery
- Greater likelihood of infection and systemic complications
2. Importance of Early Recognition
Nurses play a central role in identifying early signs of postoperative wound dehiscence, including:
- Changes in wound edges or visible separation of wound
- Increased drainage or bleeding from the postoperative wound
- Patient complaints of sudden discomfort or a “giving way” sensation
Recognizing these signs early allows for timely intervention, preventing progression to evisceration.
3. Immediate Response to Complications
In cases where evisceration occurs, rapid action is critical. Key priorities include:
- Cover the wound with a sterile dressing to protect exposed internal organs
- Reduce strain on the abdominal wall using positioning or an abdominal binder
- Notify healthcare providers immediately, as this condition requires immediate medical attention
4. Role in Prevention
Preventive care is a major component of nursing responsibilities. Effective strategies include:
- Educating patients to avoid heavy lifting, cough, or sneeze without support
- Ensuring proper wound care and adherence to sterile techniques
- Monitoring for risk factors such as obesity, malnutrition, and poor glycemic control
5. Supporting Recovery and Healing
Nurses also contribute to long-term recovery by:
- Promoting optimal body’s healing conditions through nutrition and hydration
- Monitoring for signs of poor wound healing or delayed healing
- Assisting in advanced therapies such as negative pressure wound therapy or healing by secondary intention in complex cases
Wound Dehiscence: Definition, Types, and Pathophysiology
Wound dehiscence is a significant surgical complication characterized by the partial or complete separation of wound edges following wound closure. It most commonly occurs in the postoperative wound period after abdominal surgery, when the surgical incision has not yet regained sufficient tensile strength. As part of the broader spectrum of wound dehiscence and evisceration, it represents an early but potentially progressive failure in the healing process that can compromise the integrity of the abdominal wall and expose deeper tissue layers.
Clinically, wound dehiscence is not a single uniform condition but rather a continuum ranging from minor superficial separation to full-thickness disruption. When untreated or poorly managed, it can lead to evisceration, where internal organs become exposed through an open wound, transforming a localized issue into a medical emergency that requires immediate medical attention.
Definition and Classification of Surgical Wound Dehiscence
Definition
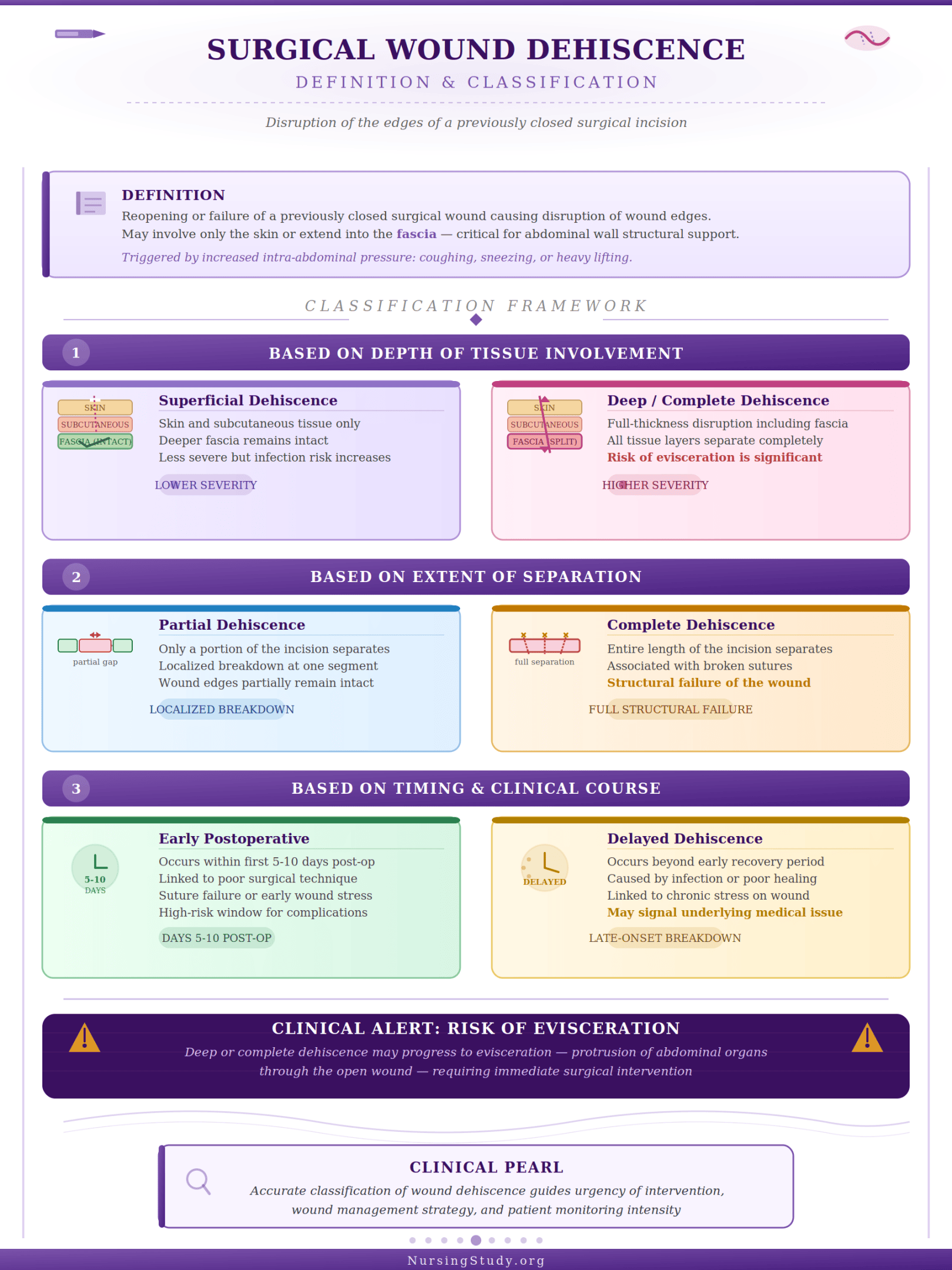
Surgical wound dehiscence refers to the reopening or failure of a previously closed surgical wound, resulting in disruption of the edges of the wound. This breakdown may involve only the skin or extend deeper into the fascia, which is critical for maintaining structural support of the abdominal wall.
A dehisced wound may present gradually or suddenly. In some cases, patients report that the wound reopens following activities that increase intra-abdominal pressure, such as a cough, sneeze, or heavy lifting. This highlights the mechanical vulnerability of the incision site during early recovery.
Classification of Wound Dehiscence
Wound dehiscence can be classified based on depth, extent, and severity:
1. Based on Depth of Tissue Involvement
- Superficial dehiscence
- Involves only the skin and subcutaneous tissue
- The deeper fascia remains intact
- Typically less severe but still increases the risk of infection
- Deep or complete wound dehiscence
- Involves full-thickness disruption, including the fascia
- May progress to complete dehiscence, where all layers separate
- Significantly increases the risk of wound failure and potential for evisceration
2. Based on Extent of Separation
- Partial dehiscence
- Only a portion of the surgical incision separates
- May appear as localized wound breakdown at one segment
- Complete wound dehiscence
- Entire length of the incision separates
- Often associated with broken sutures and structural failure
3. Based on Timing and Clinical Course
- Early postoperative wound dehiscence
- Occurs within the first 5–10 days after abdominal procedures
- Often linked to poor surgical technique, suture failure, or early stress on the wound
- Delayed dehiscence
- Occurs later due to wound infection, poor wound healing, or chronic stress
- May be associated with delayed healing or underlying medical issue
Clinical Example
A patient recovering from abdominopelvic surgeries may initially demonstrate normal healing. However, after repeated episodes of severe cough, the patient notices drainage and a small opening along the surgical site. This represents partial dehiscence, which, if not addressed, could progress to complete wound dehiscence.
Pathophysiology of Wound Dehiscence and Impaired Wound Healing
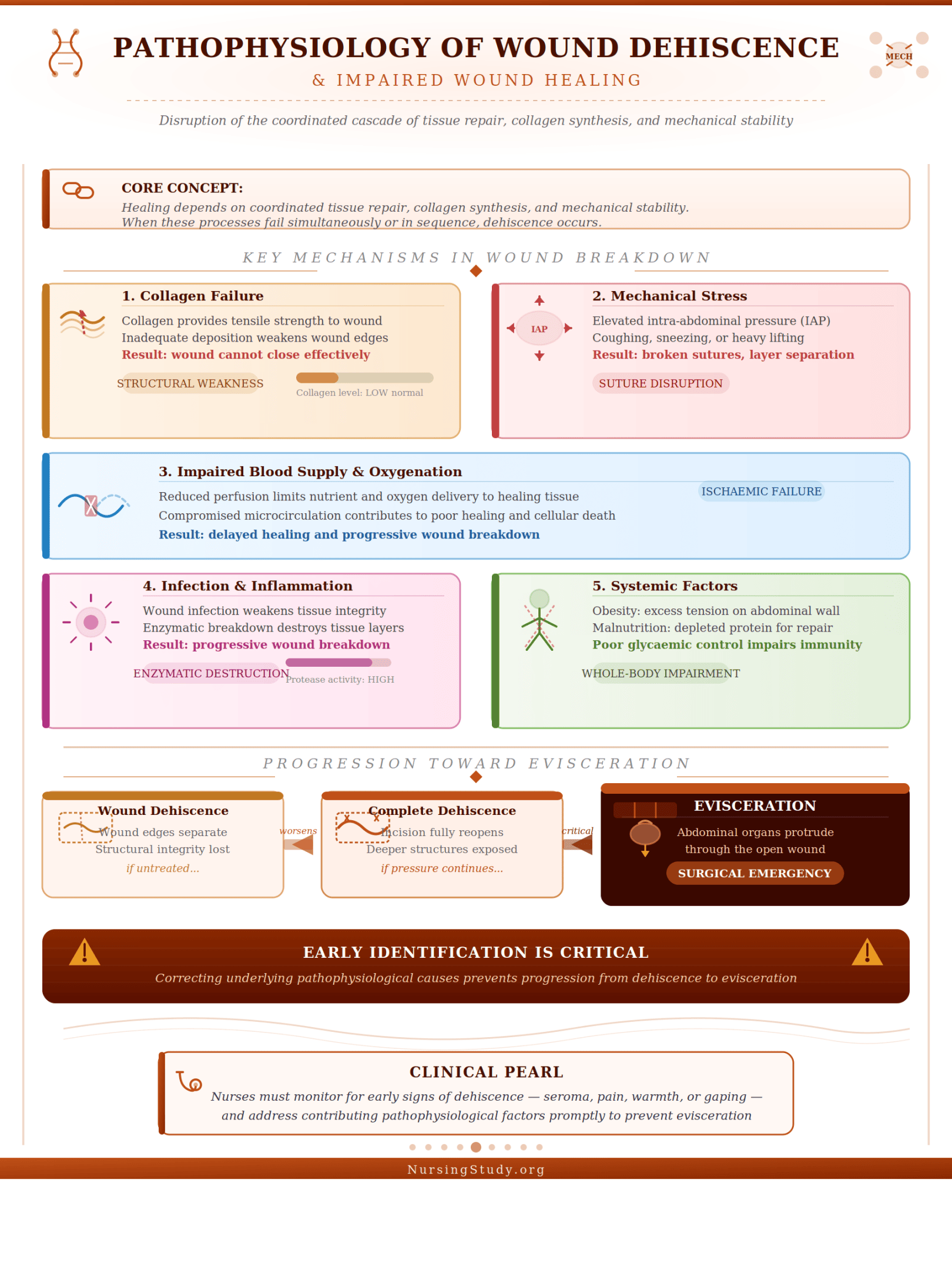
The development of wound dehiscence is fundamentally linked to disruption of the normal wound healing cascade. Healing depends on the coordinated interaction of tissue repair, collagen synthesis, and mechanical stability. When these processes fail, dehiscence occurs.
Key Mechanisms in Wound Breakdown
- Failure of Collagen Formation and Tissue Strength
- Collagen provides tensile strength to the surgical wound
- Inadequate collagen deposition weakens the edges of the wound
- Leads to inability to close the wound effectively
- Increased Mechanical Stress
- Elevated intra-abdominal pressure from cough, sneeze, or heavy lifting
- Excessive strain disrupts suture lines and may cause broken sutures
- Results in progressive separation of wound layers
- Impaired Blood Supply and Oxygenation
- Reduced perfusion limits nutrient delivery
- Contributes to poor wound healing and delayed healing
- Infection and Inflammation
- Wound infection weakens tissue integrity
- Increases the risk of infection and enzymatic breakdown of tissue
- Leads to wound breakdown and potential surgical wound dehiscence
- Systemic Factors Affecting Healing
- Obesity increases tension on the abdominal wall
- Malnutrition reduces protein availability for tissue repair
- Poor blood glucose control impairs immune function and healing
Progression Toward Evisceration
If the underlying causes are not corrected:
- A dehisced wound may worsen into complete dehiscence
- The surgical incision reopens, exposing deeper structures
- Continued stress can cause the wound to lead to evisceration, where abdominal organs begin to protrude
This progression significantly increases the need for urgent surgical intervention and advanced treatment options.
Wound Dehiscence Symptoms and Early Clinical Indicators
Early recognition of wound dehiscence symptoms is critical in preventing progression to severe wound complications such as evisceration.
Common Clinical Signs
- Local Wound Changes
- Visible separation of wound edges
- Gaping or open wound along the surgical incision
- Changes in the incision site, including swelling or redness
- Drainage and Discharge
- Sudden increase in serous or serosanguinous drainage
- Fluid leakage indicating breakdown of deeper layers
- Patient-Reported Symptoms
- Sensation that the wound reopens or “gives way”
- Pain or discomfort at the surgical site
- Signs of Infection
- Warmth, redness, and purulent discharge
- Indicators of wound infection contributing to poor wound healing
Early vs Advanced Indicators
- Early indicators
- Mild redness, slight drainage, localized wound breakdown
- Subtle changes in wound edges
- Advanced indicators
- Complete wound dehiscence
- Visible underlying tissue or fascia
- High risk of progression to evisceration
Clinical Example
Consider a patient in a medical center recovering from abdominal surgery. On day 6 postoperative, the nurse observes increased drainage and a slight gap at the surgical site. The patient reports discomfort after a bout of sneeze. These findings suggest early wound dehiscence symptoms, requiring immediate wound care, reinforcement of the dressing abdominal wound, and notification of healthcare providers to prevent worsening.
Importance of Early Detection
Prompt identification of surgical wound dehiscence allows for:
- Immediate wound care interventions
- Reduction of the risk of dehiscence progression
- Prevention of evisceration, which requires immediate medical action
Evisceration: Advanced Surgical Complication of Wound Dehiscence
Evisceration represents one of the most severe outcomes in the continuum of wound dehiscence and evisceration, occurring when a surgical wound dehiscence progresses to full-thickness disruption of the abdominal wall. In this state, the surgical incision reopens, and internal organs, particularly abdominal organs, may protrude through the open wound. This condition is universally regarded as a medical emergency that requires immediate medical attention and urgent surgical intervention.
While wound dehiscence involves the separation of wound edges, evisceration indicates a complete structural failure of the surgical site, including the fascia, which normally provides critical support to keep internal organs contained. As such, evisceration is not only a local surgical complication but also a life-threatening medical issue associated with a significantly increased mortality rate if not managed promptly.
Definition and Clinical Significance of Evisceration
Definition
Evisceration is defined as the extrusion of abdominal organs through a dehisced wound, resulting from complete wound dehiscence. This occurs when all layers of the surgical wound, including skin, subcutaneous tissue, and fascia, fail, allowing direct exposure of internal structures.
Key defining features include:
- A fully open wound at the incision site
- Visible protrusion of internal organs through the surgical incision
- Loss of integrity of the abdominal wall
Clinical Significance
The clinical importance of evisceration lies in its rapid progression and potential for severe complications:
- Threat to Organ Integrity
- Exposed abdominal organs are highly vulnerable to trauma and dehydration
- Increased risk of infection due to contamination of normally sterile tissues
- Risk of Systemic Complications
- Potential for sepsis from wound infection
- Fluid and heat loss from exposed tissues
- Increased mortality rate in untreated or delayed cases
- Impact on Recovery
- Prolonged hospitalization in a medical center
- Need for complex treatment options, including reoperation
- Delayed healing process and increased likelihood of long-term complications such as hernia, often requiring hernia repair
- Classification as a Surgical Emergency
- Unlike superficial dehiscence, evisceration is always a medical emergency
- Immediate response is required to cover the wound and protect exposed organs
Progression from Surgical Wound Dehiscence to Evisceration
The transition from surgical wound dehiscence to evisceration is typically gradual but can occur suddenly under certain conditions. Understanding this progression is essential for early recognition and prevention.
Stepwise Progression
- Initial Wound Weakness
- Poor wound healing due to malnutrition, uncontrolled blood glucose, or inadequate perfusion
- Weakening of the edges of the wound and underlying fascia
- Partial or Complete Dehiscence
- Development of a dehisced wound with visible separation of wound layers
- May begin as partial dehiscence and progress to complete wound dehiscence
- Mechanical Stress and Wound Breakdown
- Increased intra-abdominal pressure from:
- Cough
- Sneeze
- Heavy lifting
- These forces place tension on the surgical incision, leading to further wound breakdown
- Increased intra-abdominal pressure from:
- Failure of Structural Support
- Disruption of suture lines or presence of broken sutures
- Loss of fascia integrity
- Onset of Evisceration
- The surgical incision reopens completely
- Abdominal organs begin to protrude through the open wound
Clinical Example
A patient recovering from abdominal procedures develops postoperative wound dehiscence on day 7. Initially, there is mild drainage and slight separation of wound edges. Later, after a forceful cough, the patient reports a sudden tearing sensation. Upon assessment, the nurse observes that the wound reopens, and loops of intestine are visible at the surgical site. This indicates that dehiscence occurs and has now lead to evisceration, requiring urgent intervention.
Evisceration Symptoms and Emergency Warning Signs
Early recognition of evisceration symptoms is critical, as delays in treatment significantly increase the risk of wound complications and mortality.
Immediate and Obvious Signs
- Visible protrusion of abdominal organs through the open wound
- Sudden surgical incision reopens with widening gap
- Exposure of moist, pink or red tissue outside the body
Patient-Reported Symptoms
Patients may describe:
- A sudden “popping” or tearing sensation at the incision site
- Acute pain or discomfort
- Sensation of something “giving way” in the abdominal wall
Associated Clinical Findings
- Signs of wound infection (redness, discharge, odor)
- Evidence of poor wound healing or delayed healing prior to event
- Increased drainage from the postoperative wound
Emergency Warning Indicators
The following signs indicate that evisceration requires immediate medical action:
- Rapid Exposure of Internal Organs
- Any visible abdominal organs outside the body
- Signs of Systemic Instability
- Tachycardia, hypotension, or signs of shock
- High Risk of Contamination
- Loss of protective barrier of the surgical wound
- Increased risk of infection
Immediate Clinical Priorities
When evisceration is identified, urgent steps must be taken:
- Cover the wound with a sterile saline-moistened dressing abdominal wound
- Avoid attempting to push internal organs back into the abdominal cavity
- Position the patient to reduce strain on the abdominal wall
- Notify healthcare providers immediately for emergency surgical intervention
Importance of Rapid Response
Failure to act promptly can result in:
- Severe infection and sepsis
- Further wound breakdown
- Increased mortality rate
Conversely, early intervention improves outcomes and reduces complications associated with wound dehiscence and evisceration.
Wound Dehiscence vs Evisceration: Key Clinical Differences
Understanding the distinctions between wound dehiscence and evisceration is essential for accurate assessment, timely intervention, and prevention of severe wound complications following abdominal surgery. Although both conditions arise from failure of a surgical wound, they differ significantly in severity, tissue involvement, clinical presentation, and urgency of care. Recognizing these differences allows healthcare providers to respond appropriately and reduce the risk of wound deterioration and adverse outcomes.
At a broad level:
- Wound dehiscence involves the separation of wound edges after wound closure, which may be partial or complete.
- Evisceration represents a progression where the surgical incision reopens fully, allowing internal organs to protrude through the open wound, constituting a medical emergency.
Differences in Severity, Depth, and Tissue Involvement
1. Severity of the Condition
The most critical difference between wound dehiscence and evisceration lies in their severity:
- Wound dehiscence
- Considered a serious but often manageable surgical complication
- May range from superficial dehiscence to complete wound dehiscence
- Can often be stabilized with appropriate wound care and monitoring
- Evisceration
- Represents a life-threatening escalation
- Always classified as a medical emergency that requires immediate medical and surgical intervention
- Associated with a higher mortality rate if not treated promptly
2. Depth of Tissue Involvement
The extent of tissue disruption differentiates these two conditions:
- Wound dehiscence
- May involve only the skin and subcutaneous tissue (superficial dehiscence)
- In complete dehiscence, deeper layers such as the fascia are affected, but internal organs are not exposed
- Evisceration
- Involves full-thickness disruption of the surgical wound, including the fascia
- Results in loss of containment of the abdominal wall, allowing abdominal organs to be visible outside the body
3. Structural Integrity of the Surgical Wound
- In surgical wound dehiscence, the edges of the wound separate, but some structural integrity may remain
- In evisceration, there is complete wound breakdown, and the surgical incision reopens entirely
Clinical Comparison Summary
| Feature | Wound Dehiscence | Evisceration |
|---|---|---|
| Severity | Moderate to severe | Critical, life-threatening |
| Tissue involvement | Partial or full thickness | Full thickness with organ exposure |
| Fascia integrity | May be intact or disrupted | Completely disrupted |
| Organ exposure | Absent | Present (internal organs protrude) |
| Urgency | Urgent | Immediate emergency |
Differences in Clinical Presentation and Symptoms
Differences in Clinical Presentation and Symptoms
1. Wound Dehiscence Symptoms
Patients with wound dehiscence often present with early and progressive signs:
- Visible separation of wound edges
- Increased drainage from the postoperative wound
- Sensation that the wound reopens or “pulls apart”
- Localized pain at the incision site
- Signs of poor wound healing or delayed healing
- Evidence of wound infection, increasing the risk of infection
In many cases, wound dehiscence symptoms develop gradually, providing an opportunity for early intervention.
2. Evisceration Symptoms
In contrast, evisceration presents abruptly and dramatically:
- Sudden surgical incision reopens
- Visible protrusion of abdominal organs through the open wound
- Patient may report a “popping” or tearing sensation
- Rapid progression to a critical state
Additional findings may include:
- Signs of systemic instability
- Increased intra-abdominal pressure prior to the event (e.g., cough, sneeze, or heavy lifting)
3. Key Differences in Symptom Onset
- Wound dehiscence
- Gradual onset
- Progressive wound breakdown
- Often preceded by warning signs
- Evisceration
- Sudden onset
- No time for gradual deterioration
- Immediate exposure of internal organs
Clinical Example
A patient recovering from abdominal procedures develops mild drainage and slight separation of wound edges—classic signs of surgical wound dehiscence. If not addressed, and the patient experiences a forceful cough, the wound reopens completely, and loops of intestine become visible. This demonstrates how dehiscence occurs and can rapidly lead to evisceration.
Implications for Nursing Assessment and Priority Care
The differences between wound dehiscence and evisceration directly influence clinical decision-making and care priorities.
1. Assessment Priorities
For wound dehiscence:
- Inspect the surgical site for separation of wound edges
- Assess wound edges for signs of infection or tension
- Monitor drainage, color, and odor
- Evaluate contributing risk factors such as obesity, malnutrition, and poor blood glucose control
For evisceration:
- Immediately identify exposed internal organs
- Assess patient stability (vital signs, pain level)
- Recognize that the condition requires immediate medical escalation
2. Priority Nursing Interventions
In Wound Dehiscence
- Reinforce or change dressing abdominal wound using sterile technique
- Support the abdominal wall (e.g., abdominal binder)
- Minimize strain (avoid cough, sneeze, heavy lifting)
- Promote wound healing through proper wound care
- Collaborate with healthcare providers for further treatment options
In Evisceration
Immediate actions are critical:
- Protect the wound
- Cover the wound with a sterile saline-moistened dressing
- Prevent further damage
- Do not attempt to push abdominal organs back into place
- Reduce intra-abdominal pressure
- Position the patient appropriately
- Initiate emergency response
- Notify healthcare providers immediately
- Prepare for urgent surgical intervention
3. Preventive Implications
Understanding these differences also guides preventing wound dehiscence and avoiding progression to evisceration:
- Ensure proper wound closure techniques are maintained
- Monitor for early wound dehiscence symptoms
- Address modifiable risk factors such as obesity and malnutrition
- Educate patients on protecting the surgical incision
4. Impact on Long-Term Outcomes
Failure to manage wound dehiscence and evisceration effectively can result in:
- Chronic open wound or healing by secondary intention
- Development of hernia, requiring hernia repair
- Prolonged healing process and hospitalization
Risk Factors for Wound Dehiscence and Evisceration in Surgical Wounds
The development of wound dehiscence and evisceration is rarely due to a single cause. Instead, it reflects the combined effect of multiple risk factors that compromise the integrity of a surgical wound, disrupt the normal wound healing process, and increase the likelihood of wound breakdown. These factors can be broadly categorized into patient-related, surgical/technical, and postoperative contributors. Understanding how these elements interact is essential for reducing the risk of dehiscence and preventing progression to evisceration, a severe surgical complication that may lead to evisceration if early signs are missed.
Patient-Related Risk Factors Affecting Wound Healing
Patient-specific conditions play a central role in determining how effectively a postoperative wound heals. These factors influence the body’s ability to repair tissue, resist infection, and maintain the strength of the edges of the wound.
1. Nutritional Status and Metabolic Factors
- Malnutrition significantly impairs the healing process, reducing collagen synthesis and delaying granulation
- Poor nutritional intake weakens the body’s healing capacity, increasing the risk of a dehisced wound
- Uncontrolled blood glucose levels (e.g., in diabetes) impair immune function and increase the risk of infection, leading to poor wound healing
2. Obesity and Mechanical Stress
- Obesity increases tension on the abdominal wall, placing strain on the surgical incision
- Excess adipose tissue has reduced blood supply, contributing to delayed healing
- Higher baseline intra-abdominal pressure increases the likelihood of separation of wound edges
3. Chronic Medical Conditions
- Conditions such as cardiovascular disease or chronic respiratory illness can impair oxygen delivery
- Repeated cough or frequent sneeze episodes elevate intra-abdominal pressure, stressing the incision site
- Chronic illness contributes to an increased risk of wound complications
4. Age and Tissue Integrity
- Older patients often experience reduced tissue elasticity and slower wound healing
- Fragile tissues are more prone to wound reopens and surgical wound dehiscence
Clinical Example
A patient with malnutrition and poorly controlled blood glucose undergoes abdominal surgery. Despite proper wound closure, the patient develops delayed healing and a small gap at the surgical site, indicating early wound dehiscence. Without correction of underlying factors, this could progress to more severe wound complications.
Surgical Wound and Technique-Related Risk Factors
The manner in which a surgical wound is created and closed plays a critical role in determining its strength and resilience during the postoperative period.
1. Surgical Technique and Wound Closure
- Improper surgical technique can result in excessive tension on the edges of the wound
- Inadequate wound closure increases the likelihood that dehiscence occurs
- Poor alignment of tissues prevents effective healing of the skin and muscle layers
2. Suture Material and Integrity
- Weak or improperly placed suture materials may fail under stress
- Broken sutures contribute directly to wound breakdown
- Inadequate support of the fascia compromises the structural stability of the abdominal wall
3. Type and Location of Surgical Incision
- Certain surgical incision types are more prone to stress, especially in abdominal procedures
- Vertical incisions, for example, may experience greater tension compared to transverse incisions
- High-tension areas increase the risk of dehiscence and subsequent complications
4. Tissue Handling and Sterility
- Excessive tissue trauma during surgery can impair wound healing
- Failure to maintain a sterile environment increases the likelihood of wound infection
- Infection weakens tissue integrity and promotes wound breakdown
Clinical Example
During abdominopelvic surgeries, if the fascia is not adequately secured with appropriate suture technique, the deeper layers may fail. This can result in complete wound dehiscence, increasing the chance that the condition may lead to evisceration.
Postoperative Risk Factors and Complications
Even when patient and surgical factors are optimized, events during the postoperative phase can significantly influence outcomes.
1. Increased Intra-Abdominal Pressure
Activities that elevate intra-abdominal pressure place strain on the surgical wound, including:
- Persistent cough
- Forceful sneeze
- Heavy lifting or straining
These forces can cause the surgical incision reopens, especially if healing is incomplete.
2. Infection and Poor Wound Care
- Wound infection is one of the leading causes of surgical wound dehiscence
- Poor wound care, including improper dressing abdominal wound, increases contamination risk
- Non-sterile practices compromise the healing environment
3. Delayed Healing and Wound Breakdown
- Delayed healing prolongs the period during which the incision site remains vulnerable
- Continued stress on a weak wound leads to wound reopens or complete dehiscence
- Severe cases may progress to evisceration, where abdominal organs begin to protrude
4. Postoperative Complications
- Formation of an open wound requiring healing by secondary intention
- Increased likelihood of long-term complications such as hernia, requiring hernia repair
- Extended hospital stays in a medical center and need for advanced treatment options, such as negative pressure wound therapy
Clinical Example
A patient discharged after abdominal surgery resumes normal activity too soon and engages in heavy lifting. Combined with inadequate wound care, this leads to postoperative wound dehiscence, and eventually, the wound reopens completely, progressing toward evisceration.
Assessment of Surgical Wounds and Early Detection of Complications
Early and systematic assessment of a surgical wound is essential in preventing serious wound complications, particularly wound dehiscence and evisceration. Because these conditions often develop progressively, timely identification of subtle changes in a postoperative wound can significantly reduce the risk of dehiscence and prevent escalation to life-threatening outcomes. Effective assessment integrates careful inspection, patient-reported symptoms, and continuous monitoring of the healing process.
A structured approach to wound evaluation allows healthcare providers to detect early signs of wound breakdown, intervene promptly, and support optimal wound healing.
Systematic Assessment of Surgical Wound and Wound Edges
A thorough and consistent assessment of the surgical wound should be performed throughout the postoperative period, particularly following abdominal surgery, where the abdominal wall is subjected to continuous mechanical stress.
Key Components of Wound Assessment
- Inspection of the Incision Site
- Examine the surgical incision for:
- Redness, swelling, or discoloration
- Presence of an open wound or separation of wound edges
- Signs that the surgical incision reopens
- Examine the surgical incision for:
- Assessment of Wound Edges
- Evaluate the edges of the wound for:
- Approximation (are they well-aligned or separating?)
- Integrity (intact vs fragile or macerated)
- Evidence of superficial dehiscence or deeper disruption
- Evaluate the edges of the wound for:
- Evaluation of Wound Drainage
- Monitor the type, amount, and odor of drainage:
- Serous or serosanguinous fluid may indicate early wound dehiscence
- Purulent drainage suggests wound infection, increasing the risk of infection and poor wound healing
- Monitor the type, amount, and odor of drainage:
- Palpation of Surrounding Tissue
- Assess for warmth, tenderness, or fluctuance
- Detect underlying collections that may contribute to wound breakdown
- Dressing and Wound Care Evaluation
- Ensure appropriate dressing abdominal wound technique
- Confirm that wound care is performed using sterile methods
- Identify any issues in wound care that may increase the risk of wound complications
Structured Assessment Approach (Example)
A practical step-by-step method for evaluating a postoperative wound:
- Step 1: Inspect the incision site for visible abnormalities
- Step 2: Assess wound edges for alignment and integrity
- Step 3: Evaluate drainage and signs of wound infection
- Step 4: Ask the patient about symptoms (pain, pressure, or sensation of tearing)
- Step 5: Document findings and communicate concerns to healthcare providers
Clinical Example
A patient recovering from abdominal procedures is assessed on day 5 postoperative. The nurse notes slight redness and minimal drainage but also observes that the edges of the wound are beginning to separate. This early detection of surgical wound dehiscence allows for prompt reinforcement of the dressing abdominal wound and preventive measures to close the wound effectively.
Recognizing Wound Dehiscence Symptoms and Progression
Early recognition of wound dehiscence symptoms is critical in preventing progression to more severe complications such as evisceration. These symptoms may be subtle initially but tend to worsen if underlying causes are not addressed.
Early Signs of Wound Dehiscence
- Slight separation of wound edges
- Increased serous drainage from the surgical site
- Mild discomfort or pulling sensation at the incision site
- Evidence of poor wound healing or delayed healing
Progressive Signs
As dehiscence occurs, symptoms may become more pronounced:
- Visible wound breakdown along the surgical incision
- Partial opening (partial dehiscence) or complete separation (complete dehiscence)
- Increased drainage or bleeding
- Signs of wound infection, including redness, warmth, and discharge
Advanced Indicators
- A fully dehisced wound with exposure of deeper tissue layers
- Failure of suture lines or presence of broken sutures
- Inability to maintain effective wound closure
Clinical Example
A patient reports a sudden “pulling” sensation after a bout of cough. On examination, the nurse identifies a widening gap at the surgical incision, indicating that dehiscence occurs. Immediate wound care and reduction of intra-abdominal pressure help prevent further deterioration.
Monitoring for Signs of Evisceration and Severe Complication
While wound dehiscence may develop gradually, evisceration often occurs suddenly and represents a critical escalation. Continuous monitoring is essential to detect early warning signs and initiate emergency management.
Early Warning Signs of Impending Evisceration
- Rapid worsening of wound dehiscence symptoms
- Increasing separation of wound layers
- Bulging at the incision site, suggesting pressure beneath the abdominal wall
- History of stress events (e.g., sneeze, heavy lifting, or persistent cough)
Signs of Established Evisceration
- Sudden surgical incision reopens
- Visible protrusion of abdominal organs through the open wound
- Moist, exposed tissue at the surgical site
- Patient reports a tearing or “giving way” sensation
Emergency Indicators
The following findings indicate a medical emergency that requires immediate medical action:
- Exposure of Internal Organs
- Visible loops of intestine or other abdominal organs
- Loss of Wound Integrity
- Complete failure of the surgical wound and fascia
- Signs of Systemic Instability
- Hypotension, tachycardia, or signs of shock
Immediate Nursing Priorities
When evisceration is suspected or confirmed:
- Cover the wound with a sterile, saline-moistened dressing
- Avoid manipulating or pushing internal organs back into the abdominal cavity
- Reduce strain on the abdominal wall (e.g., positioning or use of an abdominal binder)
- Notify healthcare providers immediately for urgent surgical intervention
Clinical Example
A patient in a medical center recovering from abdominal surgery suddenly reports severe pain after a forceful sneeze. Upon assessment, the nurse observes that the wound reopens, and abdominal organs are visible. This confirms evisceration, requiring immediate action to protect the open wound and prepare for emergency surgery.
Importance of Early Detection and Continuous Monitoring
Consistent assessment of the postoperative wound allows for:
- Early identification of surgical wound dehiscence
- Reduction in progression to evisceration
- Improved wound healing outcomes
- Decreased need for extensive treatment options, such as negative pressure wound therapy
Management of Wound Dehiscence in Clinical Practice
Effective management of wound dehiscence is essential to restore the integrity of the surgical wound, support the healing process, and prevent progression to evisceration. Because surgical wound dehiscence can range from mild superficial dehiscence to complete wound dehiscence, management strategies must be individualized based on severity, presence of infection, and patient-related risk factors such as obesity, malnutrition, and poor blood glucose control.
The primary goals of management include:
- Stabilizing the postoperative wound and preventing further separation of wound edges
- Promoting optimal wound healing and tissue regeneration
- Reducing the risk of infection and additional wound complications
- Preventing progression that may lead to evisceration
Immediate Nursing Interventions for Wound Dehiscence
Prompt and appropriate action when wound dehiscence symptoms are identified can significantly improve outcomes and reduce the likelihood of severe surgical complication.
1. Protecting the Wound and Preventing Further Breakdown
- Reinforce or replace the existing dressing abdominal wound using sterile technique
- Ensure the open wound is protected from contamination
- If drainage is present, apply absorbent dressings to manage exudate
2. Reducing Mechanical Stress on the Incision Site
- Position the patient to minimize strain on the abdominal wall (e.g., semi-Fowler’s position)
- Encourage splinting of the surgical incision during cough or sneeze
- Avoid activities that increase intra-abdominal pressure, such as heavy lifting
3. Supporting Structural Integrity
- Apply an abdominal binder to provide external support to the surgical wound
- Monitor for signs of wound reopens or worsening wound breakdown
4. Monitoring and Early Escalation
- Assess for progression from partial dehiscence to complete dehiscence
- Monitor for signs of wound infection, including redness, discharge, or odor
- Notify healthcare providers promptly for further evaluation and treatment options
5. Patient Education and Engagement
- Instruct patients on proper wound care techniques
- Emphasize the importance of avoiding strain on the incision site
- Educate on recognizing early wound dehiscence symptoms
Clinical Example
A patient develops mild surgical wound dehiscence on day 5 after abdominal surgery. The nurse reinforces the dressing abdominal wound, applies an abdominal binder, and educates the patient to support the incision during cough. These early interventions help prevent progression to complete wound dehiscence.
Wound Care Strategies to Promote Wound Healing
Effective wound care is central to managing a dehisced wound and facilitating optimal wound healing, particularly when primary wound closure is no longer feasible.
1. Maintaining a Clean and Sterile Environment
- Use sterile technique during dressing changes
- Prevent contamination to reduce the risk of infection
- Regularly assess for signs of wound infection
2. Dressing Selection and Management
- Choose appropriate dressings based on wound characteristics:
- Moist dressings to support granulation
- Absorbent dressings for high exudate
- Ensure proper dressing abdominal wound to protect the edges of the wound
3. Advanced Wound Care Techniques
- Negative pressure wound therapy may be used to:
- Promote tissue perfusion
- Remove excess fluid
- Enhance wound healing and reduce wound breakdown
4. Supporting Healing by Secondary Intention
- In cases where the wound cannot be immediately closed:
- Allow healing by secondary intention
- Encourage formation of granulation tissue
- Gradually close the wound over time
5. Addressing Systemic Factors
- Optimize nutrition to support the body’s healing
- Manage blood glucose to reduce delayed healing
- Address malnutrition and other underlying medical issue
Clinical Example
A patient with a large open wound following complete wound dehiscence is managed with negative pressure wound therapy. Over time, healthy granulation tissue develops, allowing gradual healing and reducing the need for immediate surgical intervention.
Conservative vs Surgical Management of Surgical Wound Dehiscence
The decision between conservative and surgical management depends on the severity of surgical wound dehiscence, presence of infection, and overall patient condition.
1. Conservative Management
Conservative approaches are appropriate for:
- Superficial dehiscence or small areas of partial dehiscence
- Absence of exposed internal organs
- Stable patients without severe infection
Key Components
- Regular wound care and dressing changes
- Monitoring of wound edges and healing progress
- Use of negative pressure wound therapy when indicated
- Supportive measures (e.g., abdominal binder, activity restriction)
Outcomes
- Gradual healing through secondary intention
- Reduced need for immediate surgical intervention
2. Surgical Management
Surgical intervention is required in more severe cases, including:
- Complete wound dehiscence involving the fascia
- Failure of conservative measures
- Presence of wound infection or extensive wound breakdown
- High risk that the condition may lead to evisceration
Surgical Options
- Re-approximation and reinforcement of the surgical incision
- Use of advanced closure techniques to strengthen the abdominal wall
- Placement of new suture materials to restore structural integrity
3. Preventing Recurrence
Following either approach, prevention remains critical:
- Address underlying risk factors such as obesity and malnutrition
- Reinforce proper wound care practices
- Educate patients to avoid heavy lifting, cough, and activities that increase intra-abdominal pressure
Clinical Example
A patient with complete wound dehiscence and broken sutures following abdominopelvic surgeries undergoes urgent surgical intervention to re-close the surgical wound. Postoperatively, strict wound care, use of an abdominal binder, and monitoring for wound dehiscence symptoms help prevent recurrence.
Emergency Management of Evisceration
Evisceration is a critical endpoint in the spectrum of wound dehiscence and evisceration, marked by complete wound dehiscence and extrusion of abdominal organs through an open wound. It represents a time-sensitive surgical complication that requires immediate medical action to prevent contamination, ischemic injury to exposed tissues, and rapid clinical deterioration. Management priorities center on:
- Protecting exposed internal organs
- Reducing further intra-abdominal pressure and mechanical stress
- Preventing wound infection and additional wound breakdown
- Expediting definitive surgical intervention
Because the surgical incision reopens fully in this scenario, bedside care must be decisive, standardized, and coordinated with rapid escalation to the surgical team.
Immediate Nursing Response to Evisceration
The first minutes following identification of evisceration are crucial. The goals are to cover the wound, preserve tissue viability, and prevent further damage.
1. Protect the Open Wound and Exposed Organs
- Cover the wound immediately with a sterile, saline-moistened dressing abdominal wound
- Use non-adherent material to avoid trauma to abdominal organs
- Keep the dressing moist to prevent desiccation of tissues and support the healing process
Rationale: Exposed internal organs are highly susceptible to contamination and drying, both of which increase the risk of infection and worsen outcomes.
2. Do Not Manipulate the Protruding Organs
- Do not attempt to push organs back into the abdominal cavity
- Avoid applying pressure to the open wound
Rationale: Manipulation can cause further injury, compromise blood supply, and increase contamination risk.
3. Position the Patient to Reduce Strain
- Place the patient in a low Fowler’s or supine position with knees slightly flexed
- This reduces tension on the abdominal wall and lowers intra-abdominal pressure
4. Control Contributing Triggers
- Encourage the patient to splint the surgical incision during cough or sneeze
- Avoid heavy lifting or any straining
- Administer prescribed analgesia to limit reflex increases in intra-abdominal pressure
5. Rapid Communication and Escalation
- Notify healthcare providers and the surgical team immediately
- Activate emergency protocols within the medical center
- Prepare the patient for urgent transfer to the operating room
Clinical Example
A patient on day 6 postoperative after abdominal surgery experiences a forceful cough, followed by a sudden tearing sensation. On assessment, the surgical site shows an open wound with visible bowel loops. The nurse immediately applies a sterile saline-moistened dressing, positions the patient to reduce strain, and alerts the surgical team—preventing further wound breakdown and expediting care.
Stabilization and Preparation for Surgical Intervention
Once immediate protection is in place, the focus shifts to stabilizing the patient and preparing for definitive surgical intervention.
1. Hemodynamic and Clinical Stabilization
- Monitor vital signs for signs of shock (tachycardia, hypotension)
- Establish or maintain IV access for fluids and medications
- Administer oxygen as indicated
Rationale: Evisceration can be associated with fluid loss, stress response, and increased mortality rate if instability is not addressed.
2. Infection Prevention and Asepsis
- Maintain a sterile field over the surgical wound
- Administer prescribed antibiotics if wound infection is suspected
- Minimize handling of the incision site
3. Ongoing Wound Protection
- Keep dressings moist; re-moisten as needed
- Observe the edges of the wound and the condition of exposed tissues
- Ensure the dressing remains secure without constricting the abdominal wall
4. Preparation for the Operating Room
- Keep the patient NPO (nothing by mouth)
- Verify consent and preoperative documentation as per protocol
- Prepare for rapid transport for re-closure of the surgical incision
5. Address Contributing Risk Factors
- Review factors that may have precipitated the event:
- Poor wound healing, malnutrition, or uncontrolled blood glucose
- Excessive intra-abdominal pressure (e.g., cough, sneeze)
- Possible suture failure or broken sutures
Rationale: Identifying underlying risk factors helps guide intraoperative decisions and reduces recurrence.
Postoperative Wound Care Following Evisceration Repair
After surgical repair, meticulous wound care and monitoring are essential to prevent recurrence of wound dehiscence and evisceration and to restore the integrity of the abdominal wall.
1. Monitoring the Postoperative Wound
- Inspect the new surgical wound regularly for:
- Wound dehiscence symptoms (early separation of wound edges)
- Signs of wound infection
- Evidence of poor wound healing or delayed healing
- Assess wound edges for approximation and integrity
2. Supporting Wound Healing
- Maintain appropriate dressing abdominal wound with sterile technique
- Promote granulation and tissue repair
- Use advanced modalities such as negative pressure wound therapy when indicated
In complex cases, healing may occur by secondary intention, especially if tension-free wound closure is not immediately achievable.
3. Reducing Mechanical Stress
- Apply an abdominal binder to support the abdominal wall
- Reinforce activity restrictions:
- Avoid heavy lifting
- Support the incision during cough or sneeze
4. Optimizing Systemic Healing
- Address malnutrition with adequate protein and micronutrient intake
- Control blood glucose to enhance the healing process
- Manage comorbid conditions contributing to delayed healing
5. Preventing Recurrence and Long-Term Complications
- Monitor for complications such as hernia, which may require hernia repair
- Educate patients on signs of wound reopens and when to seek care
- Continue surveillance for postoperative wound dehiscence
Clinical Example
Following repair of evisceration, a patient receives structured wound care, including negative pressure wound therapy to support granulation. With the addition of an abdominal binder and strict control of blood glucose, the surgical wound heals effectively without recurrence of surgical wound dehiscence.
Preventing Wound Dehiscence and Evisceration
Prevention of wound dehiscence and evisceration is a central goal in postoperative care, particularly following abdominal surgery, where the abdominal wall is exposed to continuous mechanical stress. Because these conditions arise from failure of the healing process, prevention requires a coordinated approach that integrates sound surgical technique, vigilant wound care, and proactive management of patient-related risk factors.
Effective prevention strategies focus on:
- Maintaining the integrity of the surgical wound and wound closure
- Supporting optimal wound healing at every stage
- Minimizing stress on the incision site
- Identifying and modifying factors that increase the risk of dehiscence
Surgical Strategies for Preventing Wound Dehiscence
The foundation of prevention begins in the operating room. Proper handling of tissues and meticulous closure techniques significantly reduce the likelihood that dehiscence occurs or progresses to evisceration.
1. Optimal Surgical Technique
- Use of precise surgical technique to minimize tissue trauma
- Gentle handling of skin and muscle layers to preserve blood supply
- Avoidance of excessive tension on the edges of the wound
Excessive tension is a key contributor to wound breakdown and increases the likelihood of surgical wound dehiscence.
2. Effective Wound Closure and Suture Selection
- Selection of appropriate suture material based on tissue type and patient condition
- Secure closure of the fascia, which is critical for maintaining the strength of the abdominal wall
- Ensuring even distribution of tension across the surgical incision
Failure of suture integrity or broken sutures can result in complete wound dehiscence, which may lead to evisceration.
3. Maintaining a Sterile Surgical Environment
- Strict adherence to sterile technique to prevent contamination
- Reduction of wound infection, a major cause of poor wound healing
4. Appropriate Incision Planning
- Selection of incision type that minimizes stress on the surgical site
- Consideration of patient-specific risk factors, such as obesity or prior abdominal procedures
Clinical Example
During abdominopelvic surgeries, careful closure of the fascia using reinforced suture techniques ensures that the surgical wound can withstand postoperative stress. This reduces the likelihood of postoperative wound dehiscence.
Nursing Role in Preventing Wound Dehiscence and Complications
Nurses play a critical role in preventing wound dehiscence by maintaining the integrity of the postoperative wound, monitoring for early wound dehiscence symptoms, and educating patients on protective behaviors.
1. Ongoing Wound Assessment
- Regular inspection of the surgical wound and wound edges
- Early identification of separation of wound or signs that the wound reopens
- Monitoring for wound infection, which increases the risk of infection and wound complications
2. Maintaining Proper Wound Care
- Use of sterile technique during dressing changes
- Appropriate dressing abdominal wound to protect the incision site
- Ensuring a clean, moist environment to promote granulation and wound healing
3. Reducing Mechanical Stress
- Educating patients to support the surgical incision during cough or sneeze
- Reinforcing avoidance of heavy lifting and straining
- Use of an abdominal binder to support the abdominal wall
4. Patient Education and Engagement
- Teaching patients to recognize early wound dehiscence symptoms
- Encouraging adherence to activity restrictions and wound care instructions
- Promoting follow-up visits at the medical center for ongoing monitoring
5. Early Intervention and Escalation
- Promptly reporting any signs of surgical wound dehiscence to healthcare providers
- Initiating preventive measures to close the wound and avoid progression to evisceration
Clinical Example
A nurse caring for a patient after abdominal surgery notices mild redness and slight separation of wound edges. By reinforcing the dressing abdominal wound, applying an abdominal binder, and limiting strain from cough, the nurse helps prevent progression to complete dehiscence.
Optimizing Wound Healing to Reduce Risk Factors
Optimizing the healing process is essential in minimizing risk factors that contribute to wound dehiscence and evisceration. This involves addressing both local wound conditions and systemic health factors.
1. Supporting the Body’s Healing Capacity
- Ensure adequate nutrition to prevent malnutrition
- Promote protein intake to support collagen synthesis and tissue repair
- Encourage hydration to maintain tissue perfusion
2. Managing Chronic Conditions
- Control blood glucose to reduce delayed healing
- Manage respiratory conditions to minimize cough and increased intra-abdominal pressure
- Address comorbidities that impair wound healing
3. Preventing Infection
- Maintain strict sterile wound care practices
- Monitor for early signs of wound infection
- Initiate timely treatment to prevent wound breakdown
4. Reducing Physical Stress on the Wound
- Limit activities that increase intra-abdominal pressure
- Educate patients on proper movement techniques after abdominal procedures
- Encourage gradual return to normal activity
5. Utilizing Advanced Therapies
- Consider negative pressure wound therapy in high-risk patients
- Support healing in complex wounds or those at risk of becoming a dehisced wound
Clinical Example
A patient with obesity and malnutrition is identified as high risk for wound complications after abdominal surgery. Through nutritional support, strict wound care, and use of an abdominal binder, the care team enhances the healing process and reduces the likelihood of postoperative wound dehiscence.
Clinical Application and Nursing Considerations
Translating knowledge of wound dehiscence and evisceration into clinical practice requires strong assessment skills, timely decision-making, and coordinated care. In real-world settings, patients rarely present with textbook findings; instead, subtle changes in a postoperative wound may signal the beginning of a serious surgical complication. Nurses must integrate clinical data, recognize patterns, and act quickly to prevent deterioration.
Effective clinical application focuses on:
- Early recognition of wound dehiscence symptoms
- Continuous evaluation of the surgical wound and wound edges
- Prompt intervention to support wound healing and prevent escalation
- Prioritization of care when complications arise
Case-Based Application of Wound Dehiscence and Evisceration
Using case scenarios helps illustrate how wound dehiscence and evisceration develop and how clinical decisions influence outcomes.
Case 1: Early Surgical Wound Dehiscence
Scenario:
A patient on day 5 postoperative after abdominal surgery reports mild discomfort at the incision site. On assessment, the nurse notes slight redness, increased drainage, and minimal separation of wound edges.
Clinical Interpretation:
- Findings suggest early wound dehiscence (likely superficial dehiscence)
- Risk factors may include obesity, malnutrition, or increased intra-abdominal pressure
Nursing Actions:
- Reinforce dressing abdominal wound using sterile technique
- Monitor for progression of wound dehiscence symptoms
- Educate the patient to support the surgical incision during cough or sneeze
- Notify healthcare providers for further evaluation
Outcome:
With timely wound care, the surgical wound stabilizes, and the healing process continues without progression to more severe wound complications.
Case 2: Progression to Complete Wound Dehiscence
Scenario:
A patient recovering from abdominopelvic surgeries develops worsening drainage and visible widening of the edges of the wound. The wound reopens, indicating complete wound dehiscence.
Clinical Interpretation:
- Indicates significant wound breakdown, possibly involving the fascia
- Increased risk that the condition may lead to evisceration
Nursing Actions:
- Protect the open wound with appropriate wound care
- Apply an abdominal binder to support the abdominal wall
- Limit activities that increase intra-abdominal pressure (e.g., heavy lifting)
- Prepare for potential surgical intervention
Outcome:
Early escalation prevents further deterioration and allows timely management to close the wound effectively.
Case 3: Evisceration as a Medical Emergency
Scenario:
A patient suddenly reports a “popping” sensation after a forceful cough. On assessment, the surgical incision reopens, and abdominal organs are visible through the open wound.
Clinical Interpretation:
- This is evisceration, a severe progression of surgical wound dehiscence
- Represents a medical emergency that requires immediate medical intervention
Nursing Actions:
- Cover the wound with a sterile saline-moistened dressing
- Avoid manipulating the internal organs
- Position the patient to reduce strain on the abdominal wall
- Notify healthcare providers immediately for urgent surgical intervention
Outcome:
Rapid response minimizes contamination and improves survival, reducing the mortality rate associated with delayed treatment.
Prioritization and Critical Thinking in Complication Management
Managing wound dehiscence and evisceration requires nurses to prioritize care based on severity, anticipate complications, and apply clinical judgment in dynamic situations.
1. Prioritization of Care
Nurses must quickly determine the urgency of the situation:
- Low priority (monitor closely):
- Mild wound dehiscence symptoms
- Minimal separation of wound edges
- Moderate priority (urgent intervention):
- Increasing drainage or wound breakdown
- Signs of poor wound healing or wound infection
- High priority (emergency):
- Complete wound dehiscence
- Visible protrusion of internal organs (evisceration)
2. Clinical Decision-Making Framework
A structured approach supports effective management:
- Assess
- Evaluate the surgical site, wound edges, and patient symptoms
- Analyze
- Identify underlying risk factors (e.g., obesity, malnutrition, elevated blood glucose)
- Act
- Initiate appropriate wound care or emergency response
- Evaluate
- Monitor outcomes and adjust interventions
3. Anticipating Complications
Critical thinking involves recognizing patterns that suggest deterioration:
- Persistent cough or sneeze increasing intra-abdominal pressure
- Evidence of wound infection leading to wound breakdown
- Signs that the wound reopens after initial improvement
Anticipation allows for preventive measures, reducing the likelihood of surgical complication progression.
4. Interdisciplinary Collaboration
Effective management requires coordination with:
- Surgeons for decisions on surgical intervention
- Nutritionists to address malnutrition
- Other healthcare providers to manage comorbidities
5. Patient-Centered Considerations
- Educate patients on protecting the incision site
- Reinforce adherence to activity restrictions
- Encourage early reporting of wound dehiscence symptoms
Clinical Insight
In a busy medical center, a nurse identifies subtle wound dehiscence symptoms in a patient who frequently experiences cough. By prioritizing early intervention and reinforcing protective measures, the nurse prevents progression to evisceration, demonstrating the impact of critical thinking in clinical practice.
Struggling with complex nursing topics?
We’ll simplify them into clear, concise, and professional assignments.
Conclusion
Wound dehiscence and evisceration represent a continuum of postoperative wound failure, ranging from early separation of wound edges to complete disruption of the abdominal wall with exposure of internal organs. Throughout this guide, it is evident that these conditions are not isolated events but the result of complex interactions between patient-related risk factors, surgical variables, and the quality of postoperative wound care.
At its core, wound dehiscence reflects a breakdown in the normal healing process, often signaled by subtle changes such as altered wound edges, increased drainage, or early wound dehiscence symptoms. When these warning signs are missed or inadequately managed, the condition can escalate, ultimately lead to evisceration, a severe surgical complication that requires immediate medical and surgical attention. This progression underscores the importance of early detection, timely intervention, and consistent monitoring of the surgical wound.
Several key insights emerge from a comprehensive understanding of wound dehiscence and evisceration:
- Prevention is foundational
Effective surgical technique, proper wound closure, and strict adherence to sterile practices significantly reduce the risk of dehiscence and subsequent complications. - Risk factors must be actively managed
Conditions such as obesity, malnutrition, and poor blood glucose control impair wound healing and increase vulnerability to wound breakdown. Addressing these factors is essential for optimizing recovery. - Assessment drives outcomes
Regular and systematic evaluation of the incision site, wound edges, and overall postoperative wound status enables early recognition of deterioration and prevents progression to more severe states. - Timely intervention is critical
Prompt wound care, appropriate use of supportive measures like an abdominal binder, and early escalation to healthcare providers can stabilize a dehisced wound and prevent further complications. - Evisceration demands immediate action
Once the surgical incision reopens and abdominal organs begin to protrude, the situation becomes a medical emergency requiring rapid protection of the open wound and urgent surgical intervention.
From a clinical perspective, the management of wound dehiscence and evisceration highlights the essential role of vigilant, knowledgeable, and proactive care. Nurses and other healthcare providers serve as the first line of defense—identifying early changes, implementing preventive strategies, and responding decisively when complications arise.
Ultimately, improving outcomes in wound dehiscence and evisceration depends on a holistic approach: combining technical precision in surgery, evidence-based wound care, patient education, and continuous clinical assessment. By integrating these elements into everyday practice, clinicians can reduce the incidence of wound complications, support effective wound healing, and ensure safer recovery for patients undergoing abdominal procedures.
Frequently Asked Questions
What is wound dehiscence?
Wound dehiscence is the partial or complete separation of a surgical wound after closure, where the wound edges reopen due to failure in the healing process.
What is an evisceration wound?
An evisceration wound is a severe complication where a surgical incision reopens completely and internal organs (usually abdominal organs) protrude through the open wound, making it a medical emergency.
What is the recommended treatment for wound dehiscence?
Treatment depends on severity but generally includes:
- Wound care with sterile dressing to protect the wound
- Reducing strain on the abdominal wall (e.g., using an abdominal binder)
- Managing infection and underlying risk factors
- In severe cases, surgical intervention to close the wound
What are 5 possible causes of wound dehiscence?
- Wound infection
- Increased intra-abdominal pressure (e.g., cough, sneeze, heavy lifting)
- Poor surgical technique or suture failure
- Malnutrition or poor wound healing
- Obesity (causing excess tension on the surgical incision)