
Understanding Pneumonia Pathophysiology and Nursing Care
Pneumonia is a multifaceted pulmonary infection that affects the lungs, leading to significant morbidity and, in severe cases, mortality. The condition arises from a complex interplay between pathogens, including bacteria, viruses, mycoplasma, and fungi, and the host immune response, resulting in alveolar inflammation, lung parenchyma involvement, and airway obstruction. These processes impair gas exchange, leading to clinical manifestations such as cough, sputum production, chest pain, dyspnea, and in severe cases, respiratory failure.
A thorough understanding of pneumonia pathophysiology and nursing care is essential for managing these processes effectively. Pneumonia may develop in otherwise healthy individuals, but certain risk factors—such as chronic conditions like chronic obstructive pulmonary disease (COPD), immunosuppression, advanced age, and hospitalization—predispose patients to more severe disease. Vulnerable populations, including those in nursing homes or requiring mechanical ventilation, are at increased risk of hospital-acquired pneumonia, ventilator-associated pneumonia, and aspiration pneumonia.
The pathophysiological mechanisms vary according to the type of pneumonia and the pathogen involved. Bacterial pneumonia often triggers an intense inflammatory response, causing pus formation, alveolar filling, and impaired oxygenation, whereas viral pneumonia, such as that caused by respiratory syncytial virus (RSV) or COVID-19, primarily disrupts the epithelial lining and may progress more subtly. Mycoplasma pneumonia and fungal infections represent additional etiologies with unique clinical and cellular manifestations. Understanding these distinctions is crucial for tailoring nursing interventions, managing secretion clearance, administering antibiotics or antivirals, and monitoring for complications.
In addition to treatment, preventive measures play a critical role in mitigating the burden of pneumonia. Strategies such as vaccination, oral care, aspiration precautions, and early mobilization reduce the risk of developing pneumonia in vulnerable populations and support overall respiratory health. Accurate assessment, timely intervention, and ongoing monitoring are vital for optimizing patient outcomes, particularly in acute care, medical-surgical nursing, and intensive care settings.
This article provides a comprehensive overview of pneumonia pathophysiology and nursing care, examining the mechanisms of disease, clinical manifestations, risk factors, nursing assessment, and targeted interventions. The inclusion of flow charts facilitates visualization of the progression from cellular inflammation to impaired pulmonary function, linking pathophysiological changes to actionable nursing care strategies. By integrating mechanistic insights with practical management approaches, this guide aims to enhance understanding of pneumonia and support evidence-based clinical practice.
Pathophysiology of Pneumonia
Cellular and Pulmonary Changes in Pneumonia
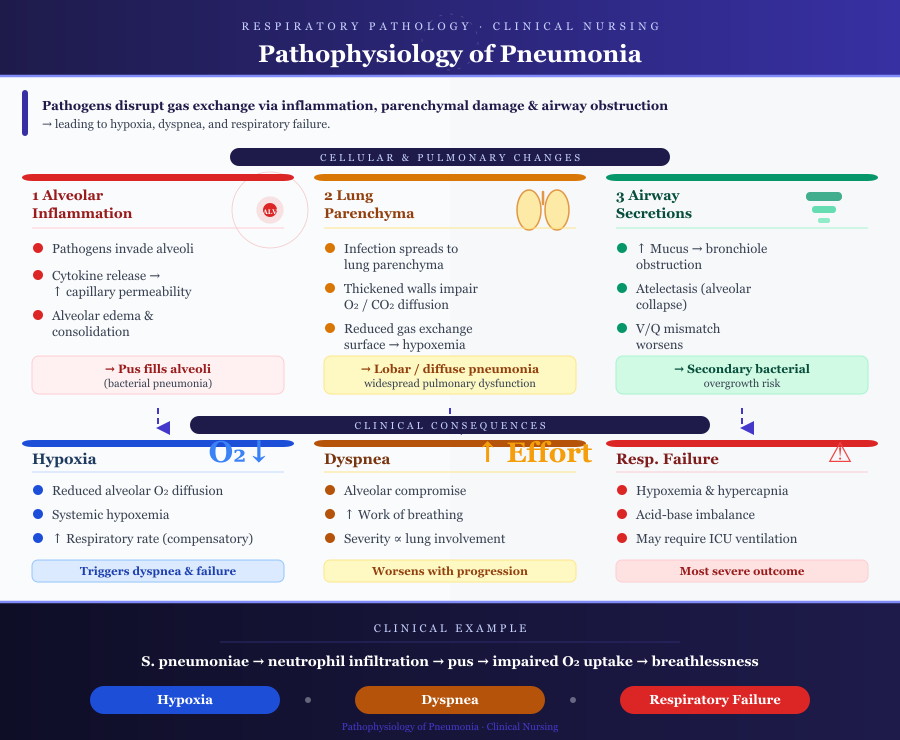
Pneumonia involves complex alterations at both the cellular and pulmonary levels, which disrupt normal gas exchange and lung function. The primary changes occur in the alveolus, lung parenchyma, and airways, leading to a cascade of physiological effects:
- Alveolar Inflammation
- Pathogens such as bacteria, viruses, mycoplasma, or fungi reach the alveoli via aspiration, inhalation, or hematogenous spread.
- The alveolar epithelium reacts by recruiting macrophages and neutrophils, which release cytokines, chemokines, and inflammatory mediators.
- This response increases capillary permeability, resulting in alveolar edema and accumulation of protein-rich exudate.
- In bacterial pneumonia, this often progresses to consolidation, where alveoli are filled with pus, neutrophils, and debris.
- Lung Parenchyma Involvement
- The infection and inflammation extend into the lung parenchyma, impairing oxygen and carbon dioxide diffusion.
- Thickened alveolar walls and exudate reduce the surface area for gas exchange, leading to hypoxemia.
- Severe involvement can affect multiple lobes (lobar pneumonia) or the entire lung (pneumonia may develop into diffuse pneumonia), resulting in widespread pulmonary dysfunction.
- Airway Secretions
- Infection triggers increased secretion and mucus production, which can obstruct bronchioles.
- Obstructed airways cause areas of alveolar collapse (atelectasis) and further ventilation-perfusion mismatch.
- Accumulated secretions can serve as a medium for secondary bacterial overgrowth, worsening the infection.
Example: In community-acquired pneumonia, Streptococcus pneumoniae colonizes alveoli, inducing neutrophil infiltration and pus formation, which impairs oxygen uptake and leads to shortness of breath.
Mechanisms of Hypoxia, Dyspnea, and Respiratory Failure
The cellular and pulmonary changes in pneumonia culminate in several critical clinical consequences:
- Hypoxia
- Reduced alveolar air space and thickened alveolar walls impede oxygen diffusion.
- Blood passing through affected regions receives insufficient oxygen, producing systemic hypoxemia.
- Hypoxia stimulates chemoreceptors, increasing respiratory rate and depth as a compensatory mechanism.
- Dyspnea
- Increased respiratory effort due to alveolar compromise causes shortness of breath.
- Airway obstruction from secretions further increases work of breathing.
- Dyspnea intensity correlates with the extent of lung involvement.
- Respiratory Failure
- Severe or untreated pneumonia can lead to acute respiratory failure.
- Features include persistent hypoxemia, hypercapnia, and acid-base imbalance.
- Patients may require mechanical ventilation in intensive care units to maintain oxygenation.
Example: In severe community-acquired pneumonia in adults, widespread consolidation can reduce PaO₂ below 60 mmHg, necessitating oxygen therapy or intubation.
Role of Pathogens in Pneumonia Etiology
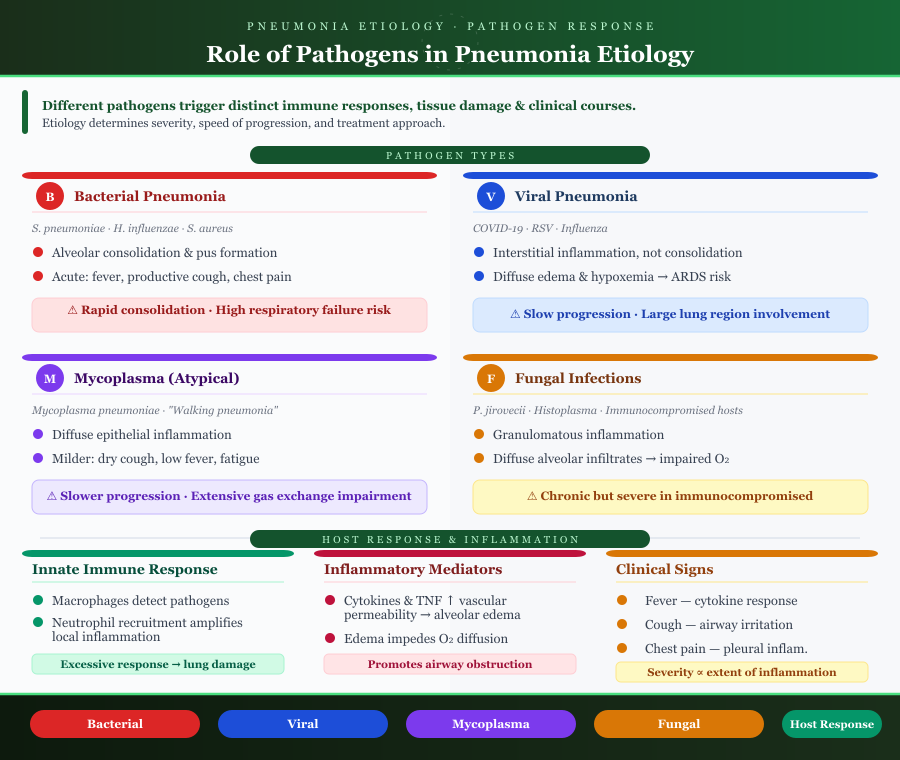
The etiology of pneumonia significantly affects its pathophysiology and clinical course. Different pathogens induce distinct immune responses and tissue damage:
- Bacterial Pneumonia
- Common bacterial causes: Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus.
- Leads to alveolar consolidation, pus formation, and intense inflammatory response.
- Often presents acutely with fever, productive cough, and pleuritic chest pain.
- Viral Pneumonia
- Caused by viruses such as COVID-19 or respiratory syncytial virus (RSV).
- Typically induces interstitial inflammation rather than alveolar consolidation.
- Can cause diffuse pulmonary involvement, edema, and hypoxemia, sometimes progressing to ARDS.
- Mycoplasma Pneumonia
- Often referred to as “atypical pneumonia.”
- Causes diffuse epithelial inflammation with minimal alveolar exudate.
- Symptoms may be milder, including dry cough, low-grade fever, and fatigue, but gas exchange can still be compromised in extensive infection.
- Fungal Infections
- Usually affect immunocompromised patients (e.g., Pneumocystis jirovecii, Histoplasma capsulatum).
- Can produce granulomatous inflammation or diffuse alveolar infiltrates, impairing oxygen diffusion.
Pathogen-Specific Severity:
- Bacterial pneumonia often leads to rapid consolidation and higher risk of respiratory failure.
- Viral or mycoplasma pneumonia may progress slowly but can affect large lung regions.
- Fungal pneumonia is often chronic but can be severe in immunocompromised hosts.
Host Response and Inflammation
The immune response to infection shapes both the clinical manifestations and severity of pneumonia:
- Innate Immune Response
- Alveolar macrophages detect pathogens and release pro-inflammatory cytokines.
- Recruitment of neutrophils and monocytes amplifies local inflammation.
- Excessive inflammatory response can contribute to lung tissue damage.
- Inflammatory Mediators
- Cytokines, interleukins, and tumor necrosis factor increase vascular permeability, leading to alveolar edema.
- Edema and exudate impede oxygen diffusion and promote airway obstruction.
- Clinical Manifestations of Inflammation
- Fever: systemic response to cytokines.
- Cough and sputum production: irritation of airway receptors and accumulation of secretions.
- Chest pain: pleural inflammation or stretching of alveolar tissues.
- Severity of symptoms often correlates with the extent of inflammation and pathogen virulence.
Example: In pneumococcal pneumonia, the combination of alveolar exudate, inflammatory edema, and pus leads to lobar consolidation visible on chest x-ray and profound hypoxia requiring close clinical monitoring.
Risk Factors and Vulnerable Populations
Understanding the risk factors that predispose individuals to pneumonia is essential for effective prevention, timely nursing assessment, and targeted nursing care. Vulnerable populations often experience more severe disease and higher rates of complications due to impaired lung function, altered immune responses, or exposure to healthcare environments that increase infection risk.
Patient-Specific Risk Factors
Pneumonia can develop in any individual, but certain patient characteristics significantly increase susceptibility. These factors include age, chronic conditions, and lifestyle or hospitalization-related influences.
1. Age-Related Risks
- Children:
- Pneumonia in children is often associated with immature immune systems and smaller airway structures, which predispose to respiratory infection.
- Infants and young children are especially susceptible to viral pathogens such as respiratory syncytial virus, which can cause viral pneumonia and compromise gas exchange.
- Example: In pediatric wards, community-acquired pneumonia in children frequently results from RSV or mycoplasma pneumonia, leading to cough, fever, and lower respiratory tract involvement.
- Elderly:
- Older adults often have diminished ciliary clearance, reduced cough reflex, and comorbidities such as chronic obstructive pulmonary disease (COPD) or heart disease, increasing the risk of developing pneumonia.
- Nursing home-acquired pneumonia is common in residents with impaired mobility or chronic illnesses, often requiring vigilant monitoring for early pneumonia symptoms.
- Nursing Home Residents:
- Residents in care facilities may have limited functional status, nutritional deficiencies, or exposure to multi-drug-resistant bacterial pneumonia, increasing morbidity and mortality.
2. Chronic Conditions
- Chronic Obstructive Pulmonary Disease (COPD):
- Patients with lung disease like COPD experience chronic airway inflammation, impaired mucociliary clearance, and altered alveolar structure, making them prone to bacterial pneumonia and acute respiratory exacerbations.
- Example: An elderly patient with COPD hospitalized for an exacerbation is at higher risk of hospital-acquired pneumonia due to compromised lung parenchyma.
- Diabetes Mellitus:
- Hyperglycemia impairs neutrophil function and cytokine response, reducing the ability to contain infections in the lower respiratory tract.
- Immunosuppression:
- Patients on immunosuppressive therapy, chemotherapy, or with HIV are highly susceptible to fungal pneumonia, viral and bacterial infections, and severe respiratory failure.
3. Lifestyle and Hospitalization
- Smoking:
- Tobacco use impairs alveolar macrophage function and ciliary clearance, facilitating pneumonia development.
- Prolonged Bed Rest:
- Immobility leads to reduced airway ventilation, promoting secretion accumulation and ventilation-perfusion mismatch, predisposing to healthcare-associated pneumonia.
- Ventilator Use:
- Mechanical ventilation introduces foreign surfaces that bypass normal airway defenses, increasing the likelihood of ventilator-associated pneumonia.
- Example: Patients in the intensive care unit on prolonged mechanical ventilation often develop pneumonia due to bacterial colonization, necessitating nursing interventions such as suctioning and oral care.
Aspiration Pneumonia
Aspiration pneumonia arises when foreign material, such as oropharyngeal secretions or gastric contents, is inhaled into the lungs, triggering acute inflammatory injury.
Mechanisms of Aspiration
- Compromised swallowing reflexes, impaired gag reflex, or neurological disorders (e.g., stroke, Parkinson’s disease) allow aspiration of contents into the lower respiratory tract.
- The aspirated material may contain bacteria (commonly oral flora) or acidic gastric contents that injure the alveolus and surrounding lung parenchyma.
Risk in Neurologically Impaired Patients
- Patients with neurological deficits are unable to clear aspirated material efficiently, leading to airway obstruction, localized inflammation, and impaired gas exchange.
- Example: An adult post-stroke patient may develop aspiration pneumonia due to accumulation of secretions, presenting with cough, fever, and increased sputum.
Resulting Lung Injury
- Aspirated material triggers an inflammatory response, attracting neutrophils and macrophages, leading to alveolar edema, consolidation, and impaired oxygenation.
- If unrecognized, severe aspiration pneumonia can progress to respiratory failure, requiring mechanical ventilation and intensive care management.
Classification of Pneumonia
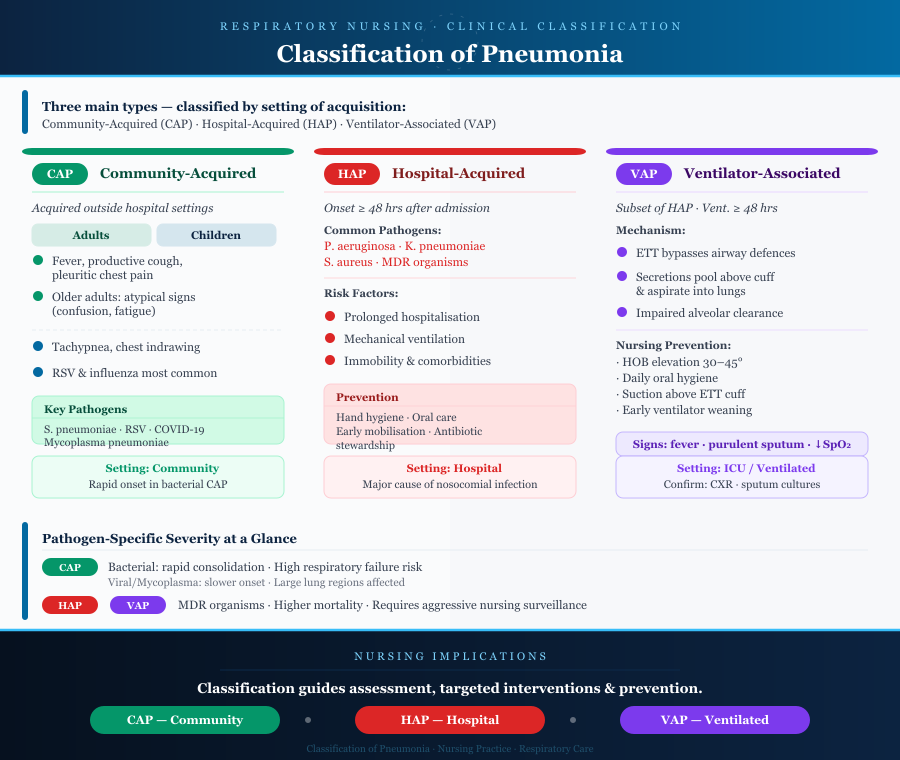
Pneumonia can be classified based on the setting of acquisition and etiological factors, which influence clinical presentation, severity, and management. Understanding these classifications guides nursing assessment, targeted nursing interventions, and prevention strategies.
Community-Acquired Pneumonia (CAP)
Community-acquired pneumonia (CAP) refers to infections of the lower respiratory tract acquired outside hospital or long-term care settings. CAP is a significant cause of morbidity and mortality worldwide.
Differences in Adults vs Children
- Adults:
- CAP in adults often presents acutely with fever, productive cough, pleuritic chest pain, and dyspnea.
- Older adults may have atypical symptoms, such as confusion or fatigue, rather than pronounced pneumonia symptoms.
- Comorbid conditions like chronic obstructive pulmonary disease, diabetes, or lung disease increase severity.
- Children:
- Pediatric CAP is commonly caused by viruses, such as respiratory syncytial virus or influenza, especially in children under five.
- Clinical signs include tachypnea, cough, chest indrawing, and fever.
- Severe CAP in children may lead to hypoxia, requiring oxygen therapy or mechanical ventilation in the intensive care unit.
Typical Pathogens and Clinical Course
- Bacterial causes:
- Streptococcus pneumoniae (pneumococcal pneumonia) is the most common pathogen in adults.
- Haemophilus influenzae and Staphylococcus aureus may also contribute.
- Viral causes:
- RSV, influenza, and SARS-CoV-2 (COVID-19) can cause viral pneumonia, often affecting alveolar and interstitial tissues.
- Atypical causes:
- Mycoplasma pneumoniae can lead to mild but prolonged pneumonia with persistent cough.
Clinical course:
- Bacterial CAP often has rapid onset, lobar consolidation, and purulent sputum production.
- Viral CAP is usually slower in onset, may affect multiple lung lobes, and can result in diffuse interstitial infiltrates.
Example: An adult with CAP caused by Streptococcus pneumoniae may present with high fever, pleuritic chest pain, productive cough with rust-colored sputum, and decreased breath sounds on auscultation.
Hospital-Acquired Pneumonia (HAP) and Nosocomial Risk
Hospital-acquired pneumonia (HAP) occurs 48 hours or more after hospital admission, not present at the time of admission. It is a major cause of morbidity in hospitalized patients and contributes to nosocomial infections.
Etiology and Risk Factors
- Etiology:
- Often caused by bacterial pathogens, including Pseudomonas aeruginosa, Klebsiella pneumoniae, and Staphylococcus aureus.
- May also involve multi-drug-resistant organisms in patients with prior antibiotic exposure.
- Risk factors in hospitalized patients:
- Prolonged hospitalization
- Mechanical ventilation
- Immobility and bed rest
- Comorbidities such as COPD, diabetes, and immunosuppression
Prevention Strategies
- Strict infection control measures, including hand hygiene and isolation protocols.
- Regular oral care and early mobilization to reduce airway colonization.
- Judicious antibiotic stewardship to prevent resistance.
- Monitoring for early signs of pneumonia, such as fever, tachypnea, cough, or changes in sputum characteristics.
Example: A post-surgical patient in the intensive care unit may develop HAP due to bacterial colonization of the lower respiratory tract while intubated, necessitating nursing interventions such as suctioning and monitoring vital signs for early detection.
Ventilator-Associated Pneumonia (VAP)
Ventilator-associated pneumonia (VAP) is a subset of hospital-acquired pneumonia occurring in patients on mechanical ventilation for 48 hours or more.
Mechanism of VAP Development
- Endotracheal tubes bypass natural airway defenses, allowing bacteria or viruses to enter the lower airways.
- Secretions can accumulate above the cuff of the endotracheal tube and aspirate into the lungs.
- Impaired alveolar clearance and lung parenchyma inflammation lead to consolidation, impaired gas exchange, and hypoxia.
Identification
- Clinical signs: new or worsening fever, purulent sputum, leukocytosis, and hypoxia.
- Respiratory assessment: changes in breath sounds, increased secretions, or dyspnea.
- Diagnostic tools: chest x-ray, sputum cultures, and blood cell counts confirm the infection.
Nursing Implications
- Preventive nursing interventions include:
- Elevating the head of the bed to reduce aspiration risk.
- Daily oral hygiene with antiseptics.
- Suctioning of secretions above the endotracheal cuff.
- Early weaning from mechanical ventilation to reduce exposure.
- Monitoring and timely reporting of changes in vital signs, oxygen saturation, or sputum is critical for early intervention.
Example: A patient in critical care medicine develops VAP after five days of mechanical ventilation. Early recognition of fever, purulent sputum, and new infiltrates on chest x-ray allows initiation of pathogen-targeted antibiotics and supportive nursing care.
Nursing Assessment of Patients with Pneumonia
Accurate nursing assessment is critical for early detection, classification, and management of pneumonia. Effective assessment allows identification of clinical deterioration, guides nursing interventions, and supports pathogen-targeted treatment. Assessment combines clinical observation, respiratory examination, and diagnostic evaluation.
Clinical Signs and Symptoms
Pneumonia manifests through a combination of pulmonary and systemic symptoms. Key observations include:
- Cough
- Often the earliest and most persistent symptom.
- Productive cough with sputum changes may indicate bacterial pneumonia, with sputum appearing purulent, rust-colored, or green.
- Dry or non-productive cough may suggest viral pneumonia or mycoplasma pneumonia.
- Example: In pneumococcal pneumonia, patients may present with a sudden onset of productive cough with rust-colored sputum.
- Sputum Changes
- Volume, color, and consistency of sputum are crucial for identifying type of pneumonia and likely pathogen.
- Thick, yellow-green sputum often points to bacterial infection.
- Clear or white sputum may indicate viral or atypical infections.
- Fever
- Results from systemic inflammatory response and release of cytokines.
- High-grade fever is common in bacterial pneumonia, whereas mild or intermittent fever is more typical of viral pneumonia.
- Chest Pain
- Pleuritic pain occurs when inflammation extends to the pleura.
- Pain is often sharp, localized, and exacerbated by cough or deep inspiration.
- Dyspnea (Shortness of Breath)
- Occurs due to impaired alveolar gas exchange, airway obstruction by secretions, and lung parenchyma involvement.
- Severe dyspnea may indicate respiratory failure, requiring urgent nursing interventions and oxygen therapy.
2. Respiratory Assessment for Pulmonary Involvement or Deterioration
A systematic respiratory assessment identifies the severity and progression of pneumonia:
- Inspection
- Observe respiratory rate, effort, use of accessory muscles, and cyanosis.
- Look for asymmetry in chest expansion suggesting lobar involvement.
- Palpation
- Assess tactile fremitus, which may increase over areas of consolidation in bacterial pneumonia.
- Percussion
- Dullness over affected lobes indicates alveolar consolidation.
- Auscultation
- Breath sounds may be diminished or altered.
- Crackles/rales indicate alveolar fluid or pus.
- Bronchial breath sounds over consolidated areas suggest lobar pneumonia.
- Monitoring for Clinical Deterioration
- Track oxygen saturation, heart rate, and respiratory rate.
- Worsening dyspnea, hypoxia, or increased purulent sputum signals progressive pulmonary involvement and potential acute respiratory failure.
Example: An adult with community-acquired pneumonia in adults may exhibit tachypnea, crackles in the lower lobes, and decreased SpO₂, requiring supplemental oxygen and nursing interventions to maintain airway clearance.
3. Diagnostic Tools
Accurate diagnosis of pneumonia requires integration of laboratory and imaging studies:
- Laboratory Tests
- Complete blood cell count: leukocytosis often indicates bacterial pneumonia, while mild leukopenia can occur in viral infections.
- Blood cultures: identify bacterial etiology in severe or systemic infections.
- Sputum Cultures
- Essential for pathogen identification and antibiotic selection.
- Helps differentiate bacterial vs viral pneumonia, guiding targeted nursing care and antibiotic therapy.
- Imaging Studies
- Chest X-ray: first-line diagnostic tool to visualize consolidation, interstitial infiltrates, or lobar involvement.
- CT scan: more sensitive for detecting early pneumonia, abscesses, or complications such as empyema.
Example: In a patient with severe community-acquired pneumonia, a chest X-ray may reveal lobar consolidation, while sputum culture identifies Streptococcus pneumoniae, allowing initiation of pathogen-specific antibiotics.
4. Flow Chart Mapping of Assessment Findings to Likely Pathogens and Severity
Flow charts are valuable tools to link clinical findings to possible causes and assess severity, facilitating nursing interventions:
- Mild symptoms (low-grade fever, dry cough, minimal dyspnea) → Likely viral or atypical pneumonia → Supportive care, monitor vital signs, encourage hydration.
- Moderate symptoms (high fever, productive sputum, pleuritic chest pain) → Likely bacterial pneumonia → Initiate antibiotic therapy, monitor oxygenation, and perform nursing interventions for airway clearance.
- Severe symptoms (tachypnea, hypoxia, altered consciousness, purulent sputum, multilobar involvement) → Severe community-acquired pneumonia or hospital-acquired pneumonia → Requires intensive care, mechanical ventilation, and close nursing assessment of respiratory failure.
Flow charts integrate patient history, clinical signs, lab results, and imaging to guide timely, evidence-based nursing care.
Nursing Care and Interventions
Effective nursing care for patients with pneumonia integrates airway management, symptom relief, pharmacological therapy, and acute care measures. Interventions focus on maintaining pulmonary function, supporting gas exchange, preventing complications, and ensuring pathogen-targeted treatment.
Airway Management and Symptom Relief
Maintaining a clear airway and alleviating symptoms is central to nursing care for patients with pneumonia.
Key Interventions
- Secretion Clearance
- Encourage coughing and deep breathing exercises to mobilize airway secretions.
- Chest physiotherapy (percussion and vibration) can help patients with thick sputum or bacterial pneumonia.
- Use suctioning in patients with impaired cough reflex or those on mechanical ventilation to prevent ventilator-associated pneumonia.
- Example: In acute bacterial pneumonia, frequent suctioning may prevent alveolar collapse and airway obstruction due to pus or mucus accumulation.
- Oxygen Therapy
- Administer oxygen to correct hypoxia from impaired gas exchange caused by alveolar inflammation and lung parenchyma involvement.
- Monitor oxygen saturation, arterial blood gases, and vital signs to guide therapy.
- Adjust delivery (nasal cannula, mask, high-flow oxygen) based on respiratory status.
- Hydration
- Adequate fluid intake helps thin secretions, facilitating expectoration.
- Monitor fluid balance, particularly in elderly patients or those with chronic lung disease.
- Positioning
- Upright or semi-Fowler’s position improves lung expansion and alveolar ventilation.
- Frequent repositioning prevents atelectasis and promotes secretion drainage.
- Techniques in Medical-Surgical Nursing for Acute Pneumonia Care
- Regular monitoring of vital signs (temperature, pulse, respiratory rate) to detect deterioration.
- Auscultation of breath sounds to assess changes in pulmonary involvement.
- Encouraging early mobilization as tolerated to improve lung perfusion and prevent hospital-acquired pneumonia.
- Patient education on breathing exercises and infection control to prevent spread.
Pharmacological Management
Targeted pharmacotherapy is essential for managing pneumonia and preventing progression to respiratory failure or sepsis.
Key Considerations
- Antibiotics
- Indicated for bacterial pneumonia, including pneumococcal pneumonia, hospital-acquired pneumonia, and ventilator-associated pneumonia.
- Selection should be pathogen-specific whenever possible, guided by sputum cultures or local antibiograms.
- Examples:
- Streptococcus pneumoniae → penicillin or ceftriaxone.
- Staphylococcus aureus → vancomycin for MRSA strains.
- Antivirals
- Used in cases of viral pneumonia, such as influenza or COVID-19, especially when initiated early.
- Supportive care remains central for most viral infections.
- Monitoring Response to Therapy
- Assess vital signs, oxygenation, sputum changes, and chest x-ray findings to determine treatment effectiveness.
- Watch for adverse drug reactions and adjust therapy accordingly.
- Importance of Pathogen-Targeted Therapy
- Bacterial pneumonia requires antibiotics, while viral pneumonia benefits from antivirals and symptomatic nursing care.
- Misuse of antibiotics in viral infections can lead to antimicrobial resistance and secondary complications.
Example: In a patient with community-acquired pneumonia in adults, culture-guided antibiotic therapy improves outcomes and reduces hospital-acquired complications.
Acute Care Measures
Preventing complications and supporting respiratory function are essential components of acute pneumonia management.
1. Preventing Complications
- Respiratory failure:
- Provide oxygen therapy, ventilatory support, and frequent respiratory assessments.
- Monitor arterial blood gases and SpO₂.
- Sepsis:
- Early recognition through vital sign monitoring, blood cultures, and labs (white blood cell count, lactate).
- Prompt antibiotic therapy and fluid resuscitation.
2. Interventions in Intensive Care and Medical-Surgical Settings
- Intensive Care Unit (ICU)
- Mechanical ventilation for patients with severe respiratory failure.
- Ventilator-associated pneumonia prevention protocols, including oral care and head-of-bed elevation.
- Continuous monitoring of vital signs, oxygenation, and lab markers.
- Medical-Surgical Nursing
- Frequent assessment of breath sounds, sputum characteristics, and oxygen saturation.
- Administration of antibiotics or antivirals, as prescribed, and monitoring therapeutic response.
- Supportive measures such as hydration, nutrition, and mobility to enhance recovery.
- Patient education on prevent pneumonia strategies, medication adherence, and early recognition of worsening symptoms.
Example: A patient with ventilator-associated pneumonia in the ICU may require suctioning, antibiotic therapy, and oxygen support, while the nurse monitors for signs of respiratory compromise or sepsis.
Prevention, Discharge Teaching, and Follow-Up
Effective management of pneumonia extends beyond acute care. Preventive nursing strategies, patient education, and structured follow-up are critical to reduce recurrence, limit complications, and improve long-term pulmonary health.
Preventive Nursing Strategies
Prevention focuses on minimizing the risk of developing pneumonia, supporting airway clearance, and reducing healthcare-associated infections.
Vaccination
- Pneumococcal vaccines significantly reduce the incidence of pneumococcal pneumonia in adults, children, and nursing home residents.
- Influenza vaccines help prevent viral pneumonia and secondary bacterial infections.
- COVID-19 vaccination reduces the risk of severe viral pneumonia and acute respiratory complications.
- Nurses play a key role in assessing vaccination status, providing education, and administering vaccines.
Oral Care
- Regular oral hygiene reduces colonization by bacteria or fungi in the oropharynx, lowering the risk of aspiration pneumonia.
- Interventions include brushing teeth, antiseptic mouthwashes, and dentures cleaning in elderly or intubated patients.
Aspiration Precautions
- For patients with neurological impairment, swallowing difficulties, or reduced consciousness, implement strategies to reduce aspiration risk:
- Elevate the head of the bed during feeding and after meals.
- Monitor for coughing or choking during oral intake.
- Provide diet modifications such as thickened liquids.
- Example: A post-stroke patient in a care facility benefits from these interventions to prevent developing aspiration pneumonia.
Infection Control
- Adherence to hand hygiene, respiratory etiquette, and isolation protocols prevents nosocomial pneumonia.
- Use of personal protective equipment when caring for patients with viral or bacterial pneumonia is essential.
Early Mobilization and Physiotherapy
- Encourage ambulation as early as tolerated to enhance lung expansion, alveolar ventilation, and airway clearance.
- Chest physiotherapy and breathing exercises improve secretion clearance and reduce the risk of hospital-acquired pneumonia.
- Example: A patient recovering from community-acquired pneumonia in adults may perform incentive spirometry exercises and short walks to prevent pulmonary complications.
Patient Education and Follow-Up
Patient-centered education ensures adherence to treatment plans, encourages early detection of complications, and promotes recovery.
Medication Adherence
- Emphasize the importance of completing the full course of antibiotics in bacterial pneumonia to prevent recurrence or resistant infections.
- Provide clear instructions for antivirals in viral pneumonia cases, highlighting timing and potential side effects.
Symptom Monitoring
- Teach patients to recognize early signs of deterioration, including:
- Increased cough or purulent sputum
- Persistent fever or chills
- Dyspnea or chest pain
- Fatigue or altered mental status in elderly patients
- Early recognition allows timely nursing assessment or medical intervention to prevent respiratory failure.
Lifestyle Adjustments
- Encourage smoking cessation to improve lung health and reduce risk of recurrent respiratory infection.
- Promote adequate hydration, nutrition, and physical activity to support immune function and pulmonary recovery.
When to Seek Medical Attention
- Patients should contact healthcare providers if they experience:
- Worsening dyspnea or hypoxia
- New or increased sputum production
- Persistent fever or chest pain
- Signs of sepsis such as hypotension, confusion, or rapid heart rate
Scheduled Follow-Up
- Arrange follow-up visits to assess lung function, symptom resolution, and treatment adherence.
- Chest X-rays may be repeated in high-risk patients to confirm resolution of infiltrates and ensure recovery of lung parenchyma.
- Example: Patients recovering from severe community-acquired pneumonia may have follow-up appointments within 1–2 weeks post-discharge for clinical evaluation and nursing guidance.
Conclusion
Pneumonia remains a significant cause of morbidity and mortality across all age groups, and understanding its pathophysiology is essential for effective nursing care. At the cellular level, alveolar inflammation, lung parenchyma involvement, and airway secretions impair gas exchange, leading to hypoxia, dyspnea, and, in severe cases, respiratory failure. The role of pathogens—whether bacterial, viral, mycoplasma, or fungal—directly influences disease severity and guides targeted interventions, including antibiotics or antivirals.
Effective nursing assessment integrates clinical signs and symptoms, such as cough, sputum changes, fever, chest pain, and dyspnea, with respiratory evaluation and diagnostic tools like chest X-ray, CT scans, and laboratory testing. Mapping these findings to probable pathogens and disease severity enhances timely intervention and improves patient outcomes.
Comprehensive nursing care and interventions encompass airway management, symptom relief, pharmacological therapy, and acute care measures, tailored to the type and severity of pneumonia. Preventive strategies—including vaccination, oral care, aspiration precautions, infection control, and early mobilization—reduce the risk of hospital-acquired and ventilator-associated pneumonia, while patient education and structured follow-up empower patients to adhere to treatment, recognize warning signs, and maintain long-term pulmonary health.
Ultimately, pneumonia pathophysiology and nursing care are intertwined. A deep understanding of the disease process, coupled with evidence-based nursing interventions, allows for early detection, effective management, and prevention of complications. By integrating assessment, care, prevention, and education, nurses play a pivotal role in reducing the burden of pneumonia and improving patient outcomes across diverse clinical settings.
Frequently Asked Questions
What is the pathophysiology of pneumonia in nursing?
The pathophysiology of pneumonia involves infection and inflammation of the lung parenchyma and alveoli, leading to impaired gas exchange. Pathogens such as bacteria, viruses, mycoplasma, or fungi invade the lower respiratory tract, triggering an immune response. This results in alveolar edema, accumulation of pus and mucus, and consolidation, which reduce oxygenation and can cause hypoxia, dyspnea, and, in severe cases, respiratory failure. In nursing, understanding this process helps guide assessment, monitoring, and targeted interventions.
What are the 7 steps in the nursing process?
The nursing process is a structured approach to patient care, consisting of:
- Assessment – Collecting patient data through history, physical exam, and diagnostics.
- Diagnosis – Identifying actual or potential health problems (e.g., impaired gas exchange).
- Outcome/Planning – Setting measurable, patient-centered goals.
- Planning Interventions – Selecting evidence-based actions to achieve goals.
- Implementation – Carrying out the nursing interventions (e.g., airway management, medications).
- Evaluation – Assessing patient response to interventions and progress toward goals.
- Revision/Modification – Updating the care plan based on evaluation and changing patient needs.
What are the four stages of pneumonia pathophysiology?
The classical four stages of pneumonia (especially in lobar bacterial pneumonia) are:
- Congestion – Vascular engorgement, alveolar fluid accumulation, and early bacterial proliferation.
- Red Hepatization – Alveoli filled with exudate, neutrophils, red blood cells, causing lung consolidation.
- Gray Hepatization – Degradation of red blood cells; alveoli remain filled with fibrin and leukocytes, giving a gray appearance.
- Resolution – Enzymatic breakdown of exudate, phagocytosis, and gradual restoration of normal lung architecture.
What is the nursing care plan for pneumonia?
A nursing care plan for pneumonia focuses on maintaining airway patency, promoting oxygenation, preventing complications, and supporting recovery:
Assessment: Monitor vital signs, breath sounds, sputum characteristics, oxygen saturation, and chest x-ray findings.
Nursing Diagnoses: Examples include:
- Impaired gas exchange
- Ineffective airway clearance
- Risk for infection
- Activity intolerance
Interventions:
- Administer oxygen therapy and ensure proper positioning for lung expansion.
- Encourage coughing, deep breathing, and hydration to clear secretions.
- Administer pathogen-targeted antibiotics or antivirals, monitor response, and watch for adverse effects.
- Promote rest, nutrition, and early mobilization to support recovery.
- Implement infection control measures and educate patients on preventive strategies and vaccination.
Evaluation: Assess for improved oxygenation, reduced fever, clear or decreased sputum, resolution of dyspnea, and patient adherence to medications and follow-up care.