
How to Read a Toco Monitor: A Complete Guide to Monitoring Contractions and Fetal Heart Rate in Labor and Delivery
Understanding how to read a toco monitor is essential for safe and effective management of labor and delivery. Accurate interpretation of uterine contraction patterns and fetal heart rate is critical for assessing fetal well-being and guiding timely interventions. The toco monitor, also known as a tocodynamometer, is an external device placed on the maternal abdomen to detect uterine activity, providing a visual representation of contraction frequency, duration, and strength of contractions. When combined with a fetal heart rate monitor, it allows healthcare providers to correlate uterine contractions with changes in the fetus’s heart rate, facilitating early detection of fetal distress, fetal hypoxia, or other complications that may compromise well-being during labor.
External monitoring using a toco monitor offers a noninvasive method to evaluate uterine contraction patterns and track the peak of the contraction, the end of the contraction, and overall contraction intensity. The toco number recorded on the monitor provides an indirect measure of contraction strength, which can be correlated with fundal palpation to improve accuracy. In situations where external monitoring is insufficient—such as in maternal obesity, hyperactive labor, or complex fetal conditions—internal monitoring using an intrauterine pressure catheter (IUPC) or a fetal scalp electrode provides more precise measurements of contraction pressure in millimeters of mercury and internal fetal heart rate. These internal tools enhance the ability to assess fetal well-being during labor and guide evidence-based interventions.
Proper interpretation of contraction patterns, fetal heart rate patterns, and monitor tracings is crucial throughout all stages of labor. By analyzing frequency of contractions, contraction duration, contraction strength, and heart rate associated with uterine contractions, clinicians can identify early signs of abnormal fetal heart rate, nonreassuring patterns, or inadequate uterine activity. Integrating data from external and internal monitors ensures that interventions—such as maternal repositioning, oxygen administration, or adjustment of labor management—are timely and appropriate, ultimately supporting both maternal and fetal health.
This guide provides a comprehensive overview of how to read a toco monitor, covering external monitoring, internal monitoring techniques, contraction interpretation, and fetal heart rate assessment. By understanding the relationship between uterine contractions, fetal heart rate, and labor progression, clinicians can optimize monitoring, interpret data accurately, and implement effective nursing interventions to maintain fetal well-being and ensure safe outcomes during labor and delivery.
Understanding the Toco Monitor and Uterine Contractions
What is a Toco Monitor and How It Works
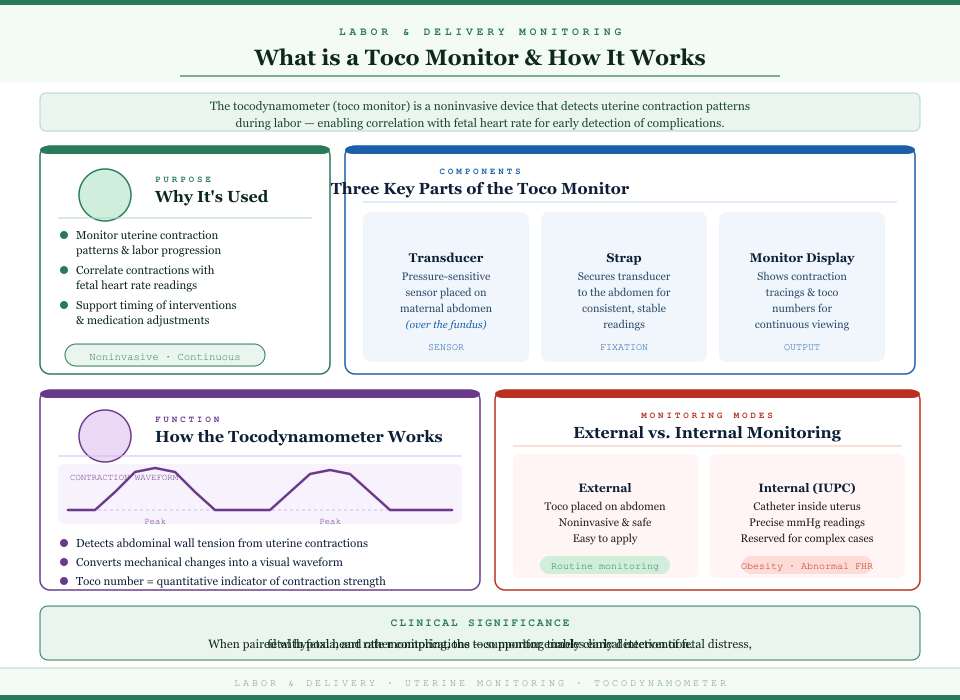
The toco monitor, also known as a tocodynamometer, is a noninvasive device used to evaluate uterine contraction patterns during labor and delivery. Its main function is to detect uterine activity and provide a visual representation of contraction frequency, duration, and intensity. When paired with a fetal heart rate monitor, it enables correlation between uterine contractions and fetal heart rate patterns, allowing early detection of fetal distress, fetal hypoxia, or other complications.
Key points about the toco monitor:
- Purpose:
- To monitor uterine contraction patterns and track labor progression.
- To assist in fetal assessment by correlating contractions with fetal heart rate.
- To support clinical decisions such as timing interventions or adjusting medications.
- Components:
- Transducer: A pressure-sensitive sensor placed on the maternal abdomen, usually over the fundus.
- Strap: Secures the transducer to ensure consistent readings.
- Monitor display: Shows contraction tracings, toco numbers, and allows for continuous observation of uterine activity.
- Function of the tocodynamometer:
- Detects changes in abdominal wall tension caused by uterine contractions.
- Converts these mechanical changes into a visual waveform on the monitor tracing.
- Provides a toco number as a quantitative indicator of contraction strength, helping clinicians assess the intensity of each labor contraction.
- External vs Internal Monitoring:
- External monitoring uses a toco monitor on the maternal abdomen; it is noninvasive, easy to apply, and safe for routine labor monitoring.
- Internal monitoring involves placing an intrauterine pressure catheter (IUPC) or fetal scalp electrode inside the uterus. This provides more precise readings of contraction pressure in millimeters of mercury and internal fetal heart rate.
- Selection considerations: Internal monitoring is typically reserved for patients with obesity, abnormal fetal heart rate patterns, or situations where external monitoring is unreliable.
How the Toco Measures Contractions
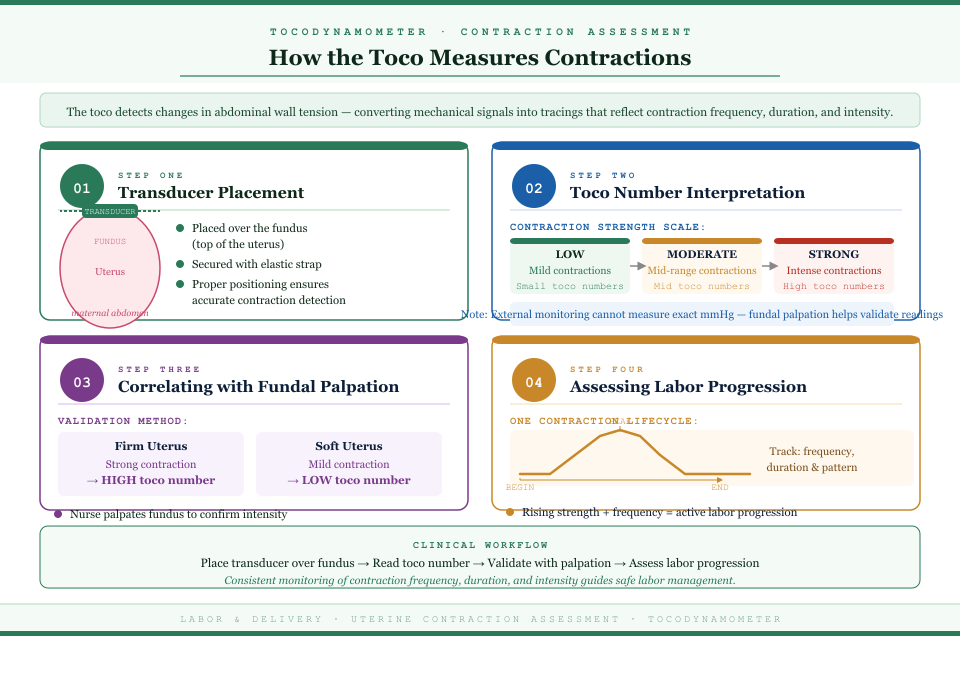
The tocodynamometer measures contractions by detecting changes in tension of the maternal abdomen:
- Transducer placement:
- The transducer is placed over the fundus, the top portion of the uterus, and secured with a strap.
- Proper positioning ensures accurate detection of uterine contractions throughout labor.
- Toco number interpretation:
- The toco number reflects the strength of the contraction on a relative scale.
- Low toco numbers indicate mild contractions, mid-range numbers indicate moderate contractions, and higher numbers reflect strong contractions.
- While external monitoring cannot measure exact uterine pressure in millimeters of mercury, fundal palpation during a contraction can validate the toco number.
- Correlating with fundal palpation:
- The nurse palpates the fundus to confirm contraction intensity.
- Example: A firm uterus with a strong contraction should correspond to a high toco number, while a softer contraction produces a lower number.
- This correlation enhances accuracy in evaluating uterine activity and guides interventions.
- Assessing labor progression:
- By monitoring one contraction to the beginning, peak, and end, clinicians can assess contraction frequency, duration, and overall contraction pattern.
- Consistent increases in contraction strength and frequency of contractions typically indicate progression from early labor to active labor.
Indications for Using an External Monitor
External fetal monitoring is often the first choice in labor due to its noninvasive nature and ease of application. Its primary indications include:
- Routine monitoring:
- For low-risk patients during the first stage of labor, to assess uterine contraction patterns and fetal heart rate.
- Labor progression assessment:
- To track contraction frequency, duration, and intensity as labor progresses.
- Provides a baseline fetal heart rate for ongoing comparison.
- Safety monitoring:
- Detects early signs of fetal distress, abnormal fetal heart rate patterns, or fetal hypoxia.
- Supports timely nursing interventions, such as maternal repositioning or oxygen administration.
Advantages of external monitoring:
- Noninvasive and low risk.
- Can be applied quickly and continuously.
- Monitors both uterine activity and fetal heart rate patterns simultaneously.
Limitations of external monitoring:
- Less accurate in patients with obesity or excess abdominal adipose tissue.
- May fail to detect subtle changes in contraction strength or internal fetal heart rate.
- In some cases, internal monitoring with an IUPC or fetal scalp electrode provides more reliable data.
Clinical example:
- A patient in active labor with normal external monitor readings may continue with routine observation.
- If fetal heart rate patterns become nonreassuring or contractions appear weak on the toco monitor, an IUPC may be inserted to measure internal uterine pressure in millimeters of mercury, allowing for precise evaluation and targeted interventions.
Interpreting Contraction Patterns on the Contraction Monitor
The contraction monitor or toco monitor is a critical tool in labor management, providing continuous visualization of uterine contractions and enabling correlation with fetal heart rate patterns. Interpreting monitor tracings accurately requires understanding not just the numbers on the screen but also how they relate to clinical findings, fundal palpation, and overall labor progression. Proper interpretation allows for early detection of abnormal uterine activity, guides nursing interventions, and ensures optimal fetal well-being during labor.
Reading Contraction Tracings
Interpreting contraction monitor waveforms involves a systematic approach:
- Identification of individual contractions:
Each contraction is represented as a rise and fall of the waveform on the monitor tracing. The start of the waveform marks the onset of uterine contraction, the peak indicates the strength of the contraction, and the return to baseline marks the end of the contraction. Accurately identifying one contraction ensures proper measurement of duration and frequency. Example: A moderate contraction lasting 50 seconds is reflected as a distinct waveform, which should align with a firm fundus upon palpation. - Evaluating contraction frequency:
Frequency is measured as the time from the start of one contraction to the start of the next. In early labor, contractions may occur every 5–10 minutes, whereas in active labor, they often occur every 2–3 minutes. A rapid succession of contractions (less than 2 minutes apart) may indicate hyperstimulation, which can compromise fetal oxygenation. - Assessing contraction duration:
Duration is calculated from the beginning to the end of a single contraction. Most active labor contractions last 45–60 seconds, though prolonged contractions exceeding 90 seconds may be considered abnormal. Persistent long contractions increase uterine pressure and can reduce placental perfusion, leading to fetal hypoxia. - Analyzing contraction intensity (strength of contraction):
The toco number provides a relative estimate of contraction strength. While external toco monitors cannot measure exact uterine pressure in millimeters of mercury, fundal palpation provides confirmation. Strong contractions usually correlate with higher toco numbers, moderate contractions with mid-range numbers, and mild contractions with low numbers. Example: A toco number of 15–20 may indicate a mild contraction, while a toco number above 50, combined with a firm fundus, reflects a strong contraction capable of advancing cervical dilation. - Observing contraction patterns over time:
Regularity, progressive increases in strength, and shortening intervals indicate normal labor progression. Irregular patterns, low amplitude, or inconsistent contraction frequency can signal inadequate uterine activity, requiring evaluation and possible intervention.
Recognizing Abnormal Uterine Activity
Abnormal uterine contraction patterns can jeopardize fetal well-being and require prompt assessment and intervention. The main abnormalities include:
- Inadequate contraction strength:
Weak or infrequent contractions may fail to produce effective cervical changes. Clinically, a low toco number combined with a soft fundus indicates insufficient contraction strength. Such cases may prolong labor, increasing the risk for fetal distress or maternal exhaustion. Nursing interventions may include augmentation with oxytocin under supervision, repositioning the mother to enhance uterine perfusion, and continuous monitoring of fetal heart rate. - Hyperstimulation or tachysystole:
Defined as more than five contractions in 10 minutes or contractions lasting longer than 90 seconds. Hyperstimulation can lead to reduced placental perfusion and abnormal fetal heart rate patterns, increasing the risk of fetal hypoxia. Interventions include maternal repositioning, discontinuation of uterotonic agents, administration of oxygen, and close observation of fetal heart rate. - Irregular or uncoordinated contraction patterns:
Contractions that are weak, too long, or irregular in frequency may reflect early labor, uterine fatigue, or inadequate stimulation. Persistent irregular patterns may compromise oxygen delivery to the fetus and require a combination of fundal palpation, monitor readings, and assessment of fetal movement to guide clinical decisions.
Integrating Toco Number with Clinical Assessment
A comprehensive evaluation of uterine contractions combines toco monitor data with physical and clinical assessment:
- Correlate with fundal palpation:
Palpation ensures the toco number accurately reflects the strength of contractions. For instance, a strong toco number with a soft fundus may indicate improper transducer placement or maternal movement affecting the reading. - Assess fetal response:
Compare contractions with fetal heart rate patterns. Decelerations during contractions or baseline variability changes may indicate fetal distress. This integration allows timely nursing interventions, such as maternal repositioning, oxygen supplementation, or notifying the obstetric team. - Evaluate labor progression:
Increasing contraction frequency, duration, and intensity should align with advancing cervical dilation and engagement of the fetal head. Lack of progression may suggest the need for augmentation or further evaluation. - Documentation and continuous monitoring:
Accurate recording of monitor tracings, toco numbers, contraction patterns, and corresponding fetal heart rate patterns ensures continuity of care and supports decision-making during labor and delivery.
Practical Example in Clinical Context
A patient in active labor exhibits contractions every 2–3 minutes with toco numbers of 40–55. Fundal palpation confirms firm contractions. The fetal heart rate monitor shows moderate variability without decelerations. This pattern suggests effective labor progression, requiring continued observation and routine interventions.
Conversely, if the same patient presents with toco numbers above 60 occurring every 1.5 minutes and repetitive late decelerations on the fetal heart rate monitor, this indicates hyperstimulation with potential fetal hypoxia, necessitating immediate nursing interventions, such as maternal repositioning, discontinuation of oxytocin, and oxygen administration.
Electronic Fetal Monitoring: Fetal Heart Rate Assessment
Electronic fetal monitoring (EFM) is a cornerstone in labor and delivery, allowing healthcare providers to continuously evaluate fetal well-being by observing fetal heart rate (FHR) patterns in relation to uterine contractions. Accurate interpretation of fetal monitor tracings is essential for identifying reassuring vs nonreassuring fetal status, guiding timely nursing interventions, and preventing fetal hypoxia or distress.
Understanding the Fetal Heart Rate Monitor
The fetal heart rate monitor is a specialized device that tracks the baby’s heart rate continuously. There are two primary types:
- External fetal monitoring:
- Uses ultrasound transducers attached to the maternal abdomen to detect fetal heart rate.
- Often paired with a toco monitor or contraction monitor to track uterine activity.
- Advantages: Noninvasive, safe for mother and fetus, can provide continuous monitoring.
- Limitations: Accuracy may decrease with maternal obesity, excessive fetal movement, or malpositioned fetal head.
- Internal fetal monitoring:
- Uses a fetal scalp electrode (FSE) attached directly to the fetal scalp.
- Provides precise fetal heart rate measurement, particularly when external monitoring is unreliable.
- Often combined with intrauterine pressure catheter (IUPC) for measuring contraction strength in mmHg.
- Advantages: Provides accurate FHR and uterine contraction data, essential in high-risk labor.
- Limitations: Invasive, requires ruptured membranes, and careful aseptic technique.
Example: In a patient with obesity and continuous fetal movement, the external fetal monitor may provide intermittent readings. Placing a fetal scalp electrode allows accurate internal fetal heart rate monitoring and continuous assessment.
Basics of Fetal Heart Rate Patterns
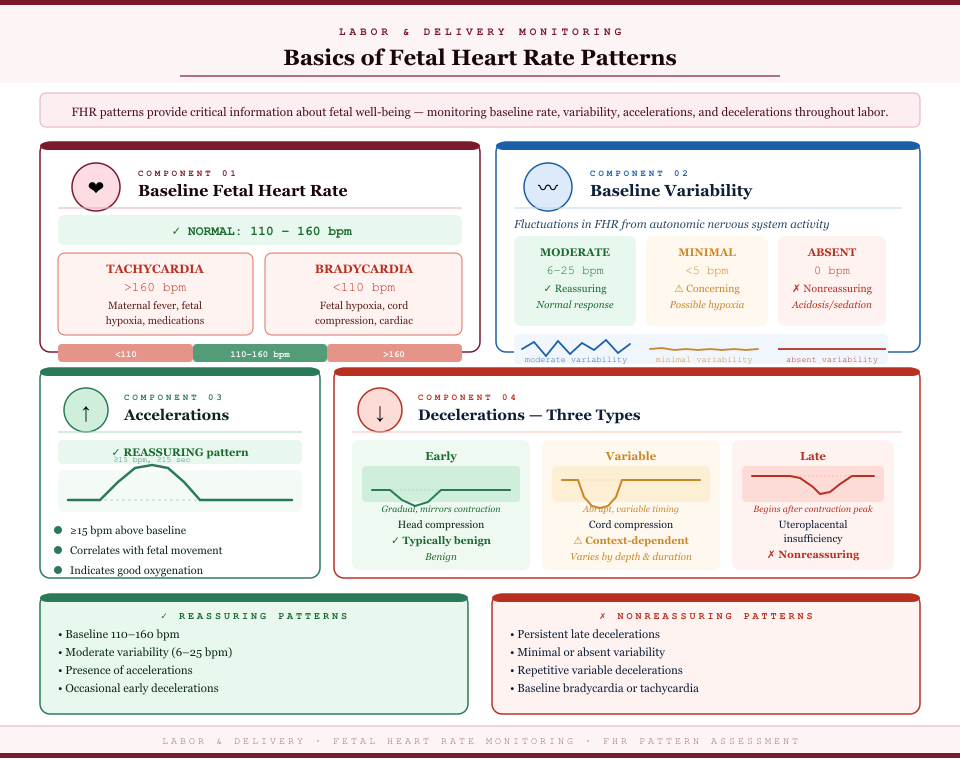
FHR patterns provide critical information about fetal well-being. Key components include:
- Baseline fetal heart rate:
- Normal: 110–160 beats per minute.
- Tachycardia: >160 bpm (may indicate maternal fever, fetal hypoxia, or medications).
- Bradycardia: <110 bpm (may indicate fetal hypoxia, cord compression, or congenital heart issues).
- Baseline variability:
- Reflects fluctuations in fetal heart rate due to autonomic nervous system activity.
- Moderate variability (6–25 bpm) is reassuring.
- Minimal (<5 bpm) or absent variability may indicate fetal hypoxia, sedation, or acidosis.
- Accelerations:
- Abrupt increases of ≥15 bpm above baseline for ≥15 seconds in term fetuses.
- Usually correlate with fetal movement and indicate adequate oxygenation.
- Reassuring and a marker of fetal well-being.
- Decelerations:
- Early decelerations: Gradual decrease mirroring contractions; typically benign, caused by fetal head compression.
- Variable decelerations: Abrupt decreases, often due to cord compression; significance depends on duration, depth, and recurrence.
- Late decelerations: Gradual decrease beginning after the contraction peak, suggesting uteroplacental insufficiency and potential fetal hypoxia.
Example: During active labor, a patient has strong contractions every 2–3 minutes. The FHR monitor shows brief accelerations during contractions but no decelerations. This pattern is reassuring, indicating the fetus is tolerating uterine activity well
Normal and Abnormal Fetal Heart Rate Patterns
Reassuring FHR patterns include:
- Baseline 110–160 bpm
- Moderate variability (6–25 bpm)
- Presence of accelerations
- Occasional early decelerations
Nonreassuring patterns suggest potential fetal compromise:
- Persistent late decelerations
- Minimal or absent variability
- Repetitive variable decelerations with slow recovery
- Baseline bradycardia or tachycardia unrelated to maternal factors
Case example: A patient in active labor exhibits repetitive late decelerations after the peak of contractions. Variability is minimal, and toco monitor tracings show strong, frequent contractions. Immediate nursing interventions (maternal repositioning, oxygen, discontinuation of oxytocin) are initiated to improve fetal oxygenation and prevent fetal hypoxia.
Correlating Fetal Heart Rate with Uterine Contraction
Understanding the relationship between contractions and FHR is essential for accurate fetal assessment:
- Effect of contractions on FHR:
- Contractions temporarily reduce uteroplacental perfusion, which can cause transient changes in FHR.
- Healthy fetuses show tolerable changes (e.g., minor decelerations or accelerations).
- Poor tolerance is indicated by late decelerations, minimal variability, or persistent bradycardia.
- Integrating Toco Monitor Data:
- Observing contraction waveforms alongside FHR allows clinicians to determine if contraction frequency, duration, and strength are affecting fetal oxygenation.
- Example: Strong contractions with late decelerations require immediate evaluation, while moderate contractions with accelerations suggest reassuring fetal status.
- Clinical Decision-Making:
- Continuous assessment allows timely nursing interventions: changing maternal position, administering oxygen, adjusting oxytocin, or preparing for operative delivery.
- Integration of external and internal monitoring ensures accuracy in high-risk scenarios.
Internal Monitoring: IUPC and Fetal Scalp Leads
While external fetal monitoring with a toco monitor provides noninvasive assessment of uterine activity and fetal heart rate, there are scenarios in labor and delivery where internal monitoring is necessary to obtain precise and reliable data. Internal monitoring involves direct measurement of uterine pressure via an intrauterine pressure catheter (IUPC) and continuous tracking of fetal heart rate using a fetal scalp electrode (FSE). These tools enhance the accuracy of fetal assessment and guide critical nursing interventions when external readings are inadequate or ambiguous.
When and Why Internal Monitoring is Used
Internal monitoring is indicated when external monitoring fails to provide accurate or continuous information about fetal well-being or uterine contractions. Common clinical indications include:
- Maternal obesity or excessive fetal movement, which may interfere with external fetal heart rate monitoring.
- High-risk labor situations requiring precise fetal heart rate patterns evaluation.
- Suspected fetal distress, including recurrent late decelerations or minimal variability.
- Labor augmentation with oxytocin, where accurate assessment of contraction strength is critical.
- Inadequate uterine activity as identified on the toco monitor, requiring measurement of contraction strength in mmHg.
Example: A patient in active labor with a history of intrauterine growth restriction exhibits recurrent late decelerations on the external fetal monitor. Placement of an FSE allows accurate internal fetal heart rate monitoring, enabling timely nursing interventions to optimize fetal oxygenation.
Difference Between Internal and External Fetal Monitoring
| Feature | External Monitoring | Internal Monitoring |
|---|---|---|
| FHR Accuracy | Subject to maternal movement, fetal position, or obesity | Directly measured from fetal scalp, highly accurate |
| Uterine Contraction Assessment | Toco monitor estimates contraction strength; qualitative | IUPC measures contraction strength quantitatively in mmHg |
| Invasiveness | Noninvasive | Invasive: requires ruptured membranes and sterile technique |
| Clinical Utility | Adequate for most low-risk labors | Essential for high-risk, ambiguous, or complicated labors |
Clinical implication: While external monitoring is generally sufficient for normal labor, internal monitoring provides more precise contraction patterns and fetal heart rate readings, crucial for detecting fetal hypoxia or distress.
Intrauterine Pressure Catheter (IUPC) Placement and Troubleshooting
The IUPC is designed to measure uterine contraction strength directly in millimeters of mercury (mmHg), providing an accurate assessment of uterine activity.
How IUPC works:
- A thin, flexible catheter is inserted through the cervix into the uterine cavity after membrane rupture.
- The catheter tip senses intrauterine pressure, which is displayed on the monitor as a waveform.
- Peak of the contraction and contraction duration are accurately recorded, allowing quantitative analysis.
Step-by-step placement:
- Prepare sterile field and gather IUPC equipment.
- Confirm membranes are ruptured and assess cervical dilation.
- Apply lubrication and gently insert the IUPC through the cervical canal into the uterine cavity.
- Advance the catheter until it is free-floating in the uterus (not against placenta or fetal parts).
- Connect the catheter to the monitor and verify contraction waveform appears on the tracing.
- Adjust depth as needed to ensure accurate readings of contraction strength.
Troubleshooting tips:
- Flat or absent waveform: catheter may be against placenta, kinked, or outside the uterus. Reposition gently.
- Erratic readings: ensure catheter tubing is free of air bubbles and properly connected to the monitor.
- Patient discomfort: confirm lubrication and gentle insertion; educate patient on sensations.
Example: In a patient with weak uterine contractions on the toco monitor, the IUPC reveals that contractions are 50–60 mmHg—adequate for labor progress—preventing unnecessary oxytocin augmentation.
Fetal Scalp Electrode Monitoring
Fetal scalp electrodes provide internal fetal heart rate monitoring, improving accuracy compared to external ultrasound monitoring.
How FSE improves accuracy:
- Directly attached to the fetal scalp, producing continuous, precise fetal heart rate readings.
- Less susceptible to maternal movement, fetal position, or obesity.
- Essential for high-risk labor, oxytocin augmentation, or ambiguous external tracings.
Placement and precautions:
- Confirm ruptured membranes and adequate cervical dilation.
- Clean fetal scalp with sterile technique.
- Attach electrode to fetal scalp using gentle rotation to ensure firm contact.
- Connect to monitor and verify FHR waveform appears.
- Monitor for potential complications: infection, scalp irritation, or bleeding.
Indications for FSE:
- Nonreassuring fetal heart rate patterns despite external monitoring.
- High-risk maternal conditions, such as preeclampsia, diabetes, or IUGR.
- Continuous monitoring during labor augmentation with oxytocin or prostaglandins.
Example: A patient exhibits recurrent variable decelerations on external monitoring during active labor. Placement of an FSE confirms the internal fetal heart rate and guides precise nursing interventions, including maternal repositioning and adjustment of uterotonic therapy.
Nursing Assessment and Interventions Using the Toco and FHR Monitors
Monitoring both uterine activity and fetal heart rate using toco monitors and fetal monitors is a critical component of safe labor and delivery. Nurses play a central role in interpreting monitor data, detecting nonreassuring patterns, implementing timely interventions, and coordinating with the obstetric team to ensure fetal well-being.
Monitoring for Nonreassuring Patterns
Nonreassuring fetal heart rate patterns indicate potential compromise in fetal oxygenation or fetal hypoxia, often reflected by abnormal fetal heart rate and uterine contractions. Nursing assessment requires continuous evaluation of fetal heart rate patterns, toco number, and uterine contraction patterns in real time.
Key assessment steps:
- Evaluate baseline fetal heart rate:
- Normal: 110–160 bpm.
- Tachycardia (>160 bpm) may indicate maternal fever, hypoxia, or fetal distress.
- Bradycardia (<110 bpm) may indicate cord compression, uteroplacental insufficiency, or profound fetal hypoxia.
- Assess variability:
- Moderate variability (6–25 bpm) indicates adequate fetal oxygenation.
- Minimal or absent variability may signal fetal compromise and requires immediate assessment.
- Identify decelerations and accelerations:
- Early decelerations are usually benign, caused by fetal head compression.
- Variable decelerations suggest cord compression.
- Late decelerations are concerning, indicating potential uteroplacental insufficiency.
- Assess contraction strength and pattern using the toco monitor:
- Strong contractions (measured via IUPC or external toco monitor) must be correlated with fetal heart rate patterns.
- Inadequate contractions may prolong labor, while excessive contractions can compromise fetal oxygenation.
Example: A patient shows late decelerations on the fetal monitor during contractions recorded by the toco monitor as strong and frequent. This pattern suggests the fetus may not be tolerating contractions well, signaling nonreassuring fetal status.
Responding to Common Monitor Alarms During Labor and Delivery
Monitor alarms alert nurses to abnormal uterine activity or fetal heart rate patterns. Effective response includes:
- Immediate assessment:
- Verify maternal and fetal status.
- Confirm monitor placement (external transducer or internal fetal scalp electrode/IUPC).
- Check for artifact due to maternal movement or electrode displacement.
- Evaluate clinical context:
- Consider maternal position, medications (e.g., oxytocin), and labor stage.
- Correlate fetal heart rate patterns with toco monitor tracings to determine if alarms indicate true compromise.
- Implement interventions:
- Notify the obstetric provider promptly for sustained nonreassuring patterns.
- Document all assessments and interventions accurately in the chart.
Example: The monitor alarm signals prolonged variable decelerations. The nurse verifies fetal scalp electrode placement, confirms contraction patterns with the toco monitor, repositions the patient, and prepares for possible obstetric intervention.
Nursing Interventions to Improve Fetal Oxygenation
When fetal distress or nonreassuring FHR patterns are detected, nurses implement interventions to optimize oxygen delivery to the fetus:
- Maternal repositioning:
- Place the patient in left lateral or semi-Fowler’s position to enhance uteroplacental perfusion and reduce cord compression.
- Oxygen therapy:
- Administer supplemental oxygen via face mask to improve maternal oxygenation and fetal oxygen delivery.
- Fluid management:
- Increase maternal IV fluids to support circulating volume and enhance uteroplacental blood flow.
- Adjust uterotonic therapy:
- Reduce or discontinue oxytocin if contractions are hyperstimulated and causing fetal heart rate decelerations.
- Continuous monitoring:
- Maintain continuous observation of FHR and uterine contractions using the toco monitor and fetal heart rate monitor.
- Document responses to interventions, including changes in toco number and fetal heart rate patterns.
Example: A patient develops late decelerations with strong contractions recorded on the toco monitor. The nurse repositions her to the left lateral side, administers oxygen, and increases IV fluids. Subsequent FHR patterns show recovery, demonstrating improved fetal well-being.
Coordination with Labor and Delivery Team Using Electronic Fetal Monitoring Data
Effective communication ensures safe outcomes:
- Share continuous fetal assessment data from toco monitors and fetal monitors with obstetric providers.
- Discuss trends in contraction frequency, duration, and intensity and corresponding FHR patterns.
- Collaborate on decisions regarding augmentation, operative delivery, or other interventions.
Example: During labor augmentation with oxytocin, a nurse observes hyperstimulation on the toco monitor with variable decelerations on the FHR monitor. The nurse promptly informs the obstetric team, and oxytocin is titrated to safe levels.
Documentation and Fetal Assessment
Accurate recording of monitor data is critical for legal, clinical, and quality purposes:
- Contraction monitor recordings:
- Document frequency, duration, and intensity of uterine contractions.
- Include toco number for external or internal monitoring readings.
- Fetal heart rate data:
- Record baseline FHR, variability, accelerations, and decelerations.
- Note any alarms, interventions, and patient responses.
- Integration into patient chart:
- Include correlation of uterine activity with fetal heart rate patterns.
- Ensure clear documentation of nursing interventions and fetal assessment findings.
Example: A labor nurse charts: “Toco monitor: contractions every 2–3 min, duration 60–70 sec, strength 50 mmHg. FHR: baseline 140 bpm, moderate variability, 1 early deceleration, no late decelerations. Interventions: maternal repositioning, oxygen 2L/min, IV fluid bolus 500 mL. FHR stabilized post-intervention.”
Differentiating True Labor from Early Labor Using Monitors
Accurate identification of true labor versus early or false labor is essential for safe labor and delivery management. Misinterpreting early labor as active labor can lead to unnecessary interventions, while failing to recognize true labor may delay appropriate monitoring and care. The use of toco monitors, fetal heart rate monitors, and careful uterine contraction assessment allows clinicians to objectively evaluate uterine activity, contraction patterns, and fetal well-being.
Contraction Monitor Patterns in True vs. Early Labor
True labor is characterized by regular, progressively stronger contractions that result in cervical changes (effacement and dilation). In contrast, early labor or false labor often presents with irregular or less intense contractions that do not advance cervical dilation.
Key distinctions using the toco monitor and contraction monitor:
- Contraction frequency and regularity:
- True labor: Contractions occur at consistent intervals, typically every 3–5 minutes during active labor, becoming progressively closer as labor advances.
- Early labor: Contractions are irregular, varying in timing and frequency, often spaced further apart (>10 minutes).
- Contraction duration and intensity:
- True labor: Contractions last longer (40–70 seconds) and gradually increase in strength of contraction, which can be quantified using toco number or, if available, IUPC readings in mmHg.
- Early labor: Contractions are shorter (30–40 seconds) and less intense, showing minimal change in uterine contraction patterns on the monitor.
- Pattern consistency:
- True labor: Contractions show a steady increase in both peak of the contraction and contraction frequency as labor progresses.
- Early labor: Contraction waveforms on the toco monitor are inconsistent, sometimes pausing entirely, and the contraction monitor tracing may not correspond with fetal heart rate changes.
Example: A patient presents with irregular contractions every 8–10 minutes, mild in intensity, with no change in cervical dilation. The toco monitor shows low-amplitude contractions, indicating early labor. In contrast, another patient with contractions every 3–4 minutes, increasing in intensity from 50–70 mmHg, shows progressive cervical dilation—a pattern consistent with true labor.
Combining FHR, Contraction, and Cervical Assessment
Monitoring uterine activity alone is insufficient to confirm labor status. Combining fetal heart rate monitoring, contraction patterns, and cervical assessment provides a more complete picture:
- Fetal heart rate monitoring:
- Changes in baseline fetal heart rate or FHR patterns may reflect fetal response to uterine contractions.
- Mild accelerations during contractions in early labor are reassuring; repetitive late decelerations during true labor may signal uterine hyperstimulation or fetal compromise, requiring intervention.
- Cervical assessment:
- Cervical dilation and effacement confirm true labor.
- Early labor typically shows minimal cervical change despite contractions.
- Monitoring cervical dilation in conjunction with toco monitor waveforms ensures that contraction intensity and frequency are physiologically effective.
- Fetal movement:
- Continuous fetal movement assessment complements fetal heart rate monitoring, indicating ongoing fetal well-being.
Example: A patient in early labor shows mild contractions on the toco monitor, baseline FHR of 140 bpm with moderate variability, and no cervical dilation. Observation continues with intermittent monitoring. Later, as contractions increase in frequency and intensity, cervical dilation progresses to 4 cm, confirming true labor.
Changes in Uterine Activity Across Stages of Labor
Uterine activity evolves throughout labor, and monitoring with a toco monitor or contraction monitor helps guide clinical decisions:
- First stage of labor (latent and active phases):
- Latent phase: Mild, irregular contractions, low toco numbers, minimal cervical change.
- Active phase: Contractions become more frequent (3–5 min), longer in duration (40–70 sec), and stronger in amplitude, correlating with progressive cervical dilation.
- Second stage of labor:
- Contractions are strong and frequent (every 2–3 minutes), typically lasting 60–90 seconds.
- Fetal heart rate monitoring is critical to detect fetal compromise during pushing efforts.
- Toco monitor readings or IUPC measurements provide quantitative data on uterine contraction patterns and strength of contractions, guiding safe pushing and maternal positioning.
- Third stage of labor:
- Contractions decrease in frequency but remain moderate in intensity to facilitate placental delivery.
- Monitoring ensures prompt detection of postpartum uterine atony or abnormal bleeding.
Example: During the second stage, a patient’s toco monitor shows strong contractions every 2 minutes, duration 70–80 seconds. The fetal monitor indicates baseline 145 bpm with moderate variability and occasional accelerations. The nurse documents contraction frequency and intensity, observes fetal movement, and prepares for safe delivery, demonstrating integration of uterine activity and fetal assessment.
How Fetal Monitor Readings Guide Interventions During the Second Stage
- Continuous FHR monitoring helps identify nonreassuring patterns during pushing.
- Adjustments in maternal positioning can improve uteroplacental perfusion and fetal oxygenation.
- Observation of toco monitor tracings ensures that contractions are effective without causing hyperstimulation, minimizing fetal compromise.
- Decisions on operative delivery, augmentation, or analgesia adjustments are informed by combined FHR, contraction monitor, and cervical assessment data.
Example: A patient in second-stage labor develops repetitive late decelerations with strong contractions on the toco monitor. The nurse repositions the patient, pauses oxytocin infusion, administers oxygen, and alerts the obstetric provider. The subsequent improvement in FHR patterns confirms effective intervention.
Conclusion
Understanding how to read a toco monitor is fundamental for safe and effective labor and delivery management. Accurate interpretation of uterine contraction patterns and fetal heart rate monitoring provides critical insight into fetal well-being during labor, enabling timely and evidence-based nursing interventions. By integrating data from external monitors, toco monitors, internal monitoring tools like IUPC and fetal scalp electrodes, and careful cervical assessment, clinicians can differentiate true labor from early labor, identify nonreassuring fetal heart rate patterns, and respond appropriately to ensure optimal outcomes.
Effective monitoring of uterine activity involves more than observing contraction frequency, duration, and strength. Nurses must correlate toco numbers with palpation at the fundus, assess fetal heart rate variability, and recognize patterns such as accelerations, decelerations, or signs of fetal hypoxia. This integration allows for informed nursing interventions—including maternal repositioning, oxygen therapy, fluid management, and adjustment of labor augmentation—to maintain fetal oxygenation and minimize risk of fetal distress.
Throughout all stages of labor, from latent contractions to the second stage, continuous monitoring of uterine contraction patterns and fetal heart rate ensures that labor progresses safely while providing early detection of complications. Accurate documentation of toco monitor tracings, fetal heart rate patterns, and corresponding nursing interventions reinforces continuity of care, supports interdisciplinary communication, and contributes to high-quality fetal assessment.
Ultimately, mastery of how to read a toco monitor empowers nurses and clinicians to make precise, timely decisions that safeguard both the fetus and the birthing parent. When applied thoughtfully, electronic fetal monitoring, in combination with skilled clinical assessment, enhances the ability to respond to labor changes effectively, promoting positive outcomes, minimizing risks, and supporting evidence-based practice in obstetric care.
Frequently Asked Questions
How to read toco on a fetal monitor?
To read a toco monitor, observe the contraction tracing on the monitor. Key points include:
- Frequency: How often contractions occur (time between the start of one contraction to the start of the next).
- Duration: How long each contraction lasts (from beginning to end of one contraction).
- Intensity/Strength: Measured as toco number on an external monitor (subjective) or in mmHg if using an IUPC.
- Peak of contraction: The highest point on the waveform indicates maximum uterine contraction strength.
How to read a fetal heart rate monitor?
To interpret a fetal heart rate (FHR) monitor:
- Identify the baseline FHR (normal: 110–160 bpm).
- Assess variability (fluctuations in baseline, moderate is 6–25 bpm).
- Look for accelerations (temporary increases) which indicate fetal well-being.
- Recognize decelerations (early, variable, or late) which may signal fetal distress.
- Correlate FHR patterns with uterine contractions on the toco monitor to determine fetal response.
What is the normal range for Toco contraction numbers?
- On an external toco monitor, normal contractions are usually displayed as 10–50 units.
- This range represents uterine tension, but the absolute value is less important than pattern, frequency, and duration.
- Internal monitoring with an IUPC measures contraction strength in millimeters of mercury (mmHg), with typical active labor contractions ranging from 50–75 mmHg.
What does toco mean on a baby heart rate monitor?
- Toco refers to uterine contractions, not the baby’s heart rate.
- On the fetal monitor, the toco channel tracks uterine activity while the FHR channel displays the baby’s heart rate.
- Reading the toco waveform alongside FHR patterns helps assess how the fetus responds to contractions and detect fetal distress if present.