
Diagnostic Criteria for Schizophrenia
Schizophrenia is chronic and complex mental health characterized by delusions, hallucinations, disorganized thinking, abnormal motor behavior, and negative symptoms. Delusions render patients’ persistent beliefs despite an agreement to the contrary or evidence (McCutcheon et al., 2020). Hallucinations entail perceived experiences that occur in the absence of external stimulus, while disorganized thinking and speech are jumbles and do not make sense. Abnormal motor behavior heightens unpredictable agitation, while negative symptoms diminish emotional expression and experience of pleasure when the disorder is active (Diagnostic Criteria for Schizophrenia).
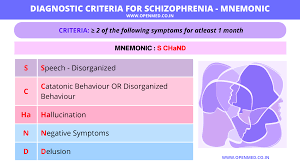
DSM-5 Criteria for Schizophrenia has A to F components that determine whether a patient should be diagnosed with a mental health condition. For Criterion A, two or more of the mentioned five symptoms should be present for one month or less if successfully treated. In this case, at least one of the symptoms should be delusions, hallucinations, or disorganized speech (Noel et al., 2020).
Moreover, In Criterion B, the level of functioning in interpersonal relations, work, or self-care remain marked below the level achieved most of the time since the onset of the disturbance. In C, continuous disturbance signs should persist for at least six months. The six-month duration should include at least one month of disturbances (or less if treated successfully) to meet Criterion A (Diagnostic Criteria for Schizophrenia).
Criterion D rules out schizoaffective disorder if no significant manic or depressive symptoms occur during the active phase or if e mood episodes occur during the active phase. In Criterion E, the disturbance is not attributed to a medical condition or physiological effects of drugs or medications. In Criterion F, a diagnosis of Schizophrenia is made if prominent hallucinations and delusions are experienced in case there is a history of childhood-onset autism or communication disorder.
Although Schizophrenia is not curable, treatment options target symptoms and prevent relapse. In addition, promotes adaptive functions allowing the patient integration into the community (Nucifora et al., 2019). Despite using other intervention strategies, such as Cognitive Behavioural Therapy (CBT), pharmacological treatment remains the cornerstone of Schizophrenia treatment, especially in the acute phase of the disease (Diagnostic Criteria for Schizophrenia).
Maroney’s (2020) report on updated pharmacotherapy treatment of Schizophrenia should suit the patients’ characteristics and preferences. The report asserts that Second Generation Antipsychotics (SGAs) such as Clozapine remain recommended first-line treatment for acute Schizophrenia. Consequently, although First Generation Antipsychotics (FGAs) remain useful for some patients.
While FGAs efficiently reduce positive symptoms such as hostility, and hallucinations, their extrapyramidal symptoms preclude their utility as first-line options. Therefore, SGAs like Clozapine remain useful in patients with poor responses to other agents or treatment-resistant Schizophrenia (Diagnostic Criteria for Schizophrenia.)
References
Maroney, M. (2020). An update on current treatment strategies and emerging agents for the management of Schizophrenia. Am J Manag Care, 26(3 Suppl), S55-S61.
McCutcheon, R. A., Marques, T. R., & Howes, O. D. (2020). Schizophrenia—an overview. JAMA psychiatry, 77(2), 201-210.
Noel, J. M., & Jackson, C. W. (2020). ASHP therapeutic position statement on the use of antipsychotic medications in the treatment of adults with Schizophrenia and schizoaffective disorder. American Journal of Health-System Pharmacy, 77(24), 2114-2132.
Nucifora Jr, F. C., Woznica, E., Lee, B. J., Cascella, N., & Sawa, A. (2019). Treatment resistant schizophrenia: Clinical, biological, and therapeutic perspectives. Neurobiology of disease, 131, 104257.