
Writing an Incident Report in Nursing: A Nurse’s Guide to Patient Safety, Quality Improvement, and Healthcare Practice in Health and Human Services
An Incident Report in Nursing is a foundational element of safe, accountable, and high-quality clinical practice. Within any healthcare setting, where multiple healthcare professionals, care providers, and staff members interact in dynamic and often high-pressure environments, the occurrence of an incident, near miss, or adverse event is not uncommon. What defines a high-performing system is not the absence of these events, but how effectively they are identified, documented, and used to improve patient safety and quality.
At its core, an Incident Report in Nursing serves as a structured and formal account of the incident, ensuring that all relevant details are captured in a clear, accurate, and concise manner. This documentation is essential not only for immediate clinical response but also for long-term quality improvement, risk management, and incident management efforts across healthcare organizations.
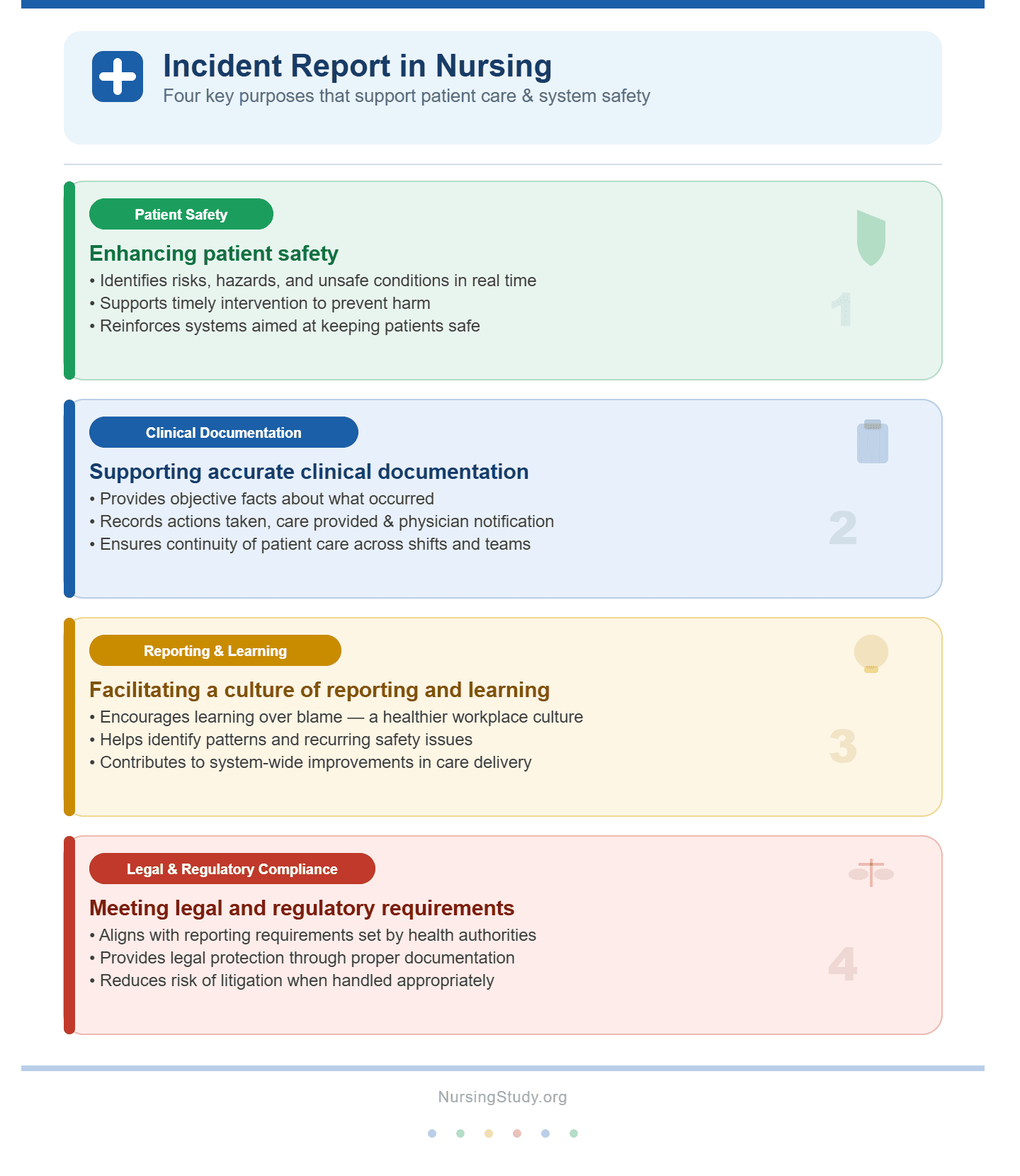
Key Purposes of an Incident Report in Nursing
An effective Incident Report in Nursing supports multiple critical functions within a healthcare facility, including:
- Enhancing Patient Safety
- Identifies risks, hazards, and unsafe conditions in real time
- Supports timely intervention to prevent harm
- Reinforces systems aimed at keeping patients safe
- Supporting Accurate Clinical Documentation
- Provides objective facts about what occurred
- Records actions taken, including care provided and physician notification
- Ensures continuity of patient care across shifts and teams
- Facilitating Reporting and Learning
- Encourages a culture of reporting and learning rather than blame
- Helps identify patterns and recurring issues
- Contributes to system-wide improvements in care delivery
- Meeting Legal and Regulatory Requirements
- Aligns with reporting requirements set by the department of health and health services
- Provides legal protection through proper documentation
- Reduces risk of litigation or legal action when handled appropriately
Understanding the Nature of Incidents in Healthcare
In practice, an incident can take many forms, and recognizing these variations is essential for effective documentation:
- Medication-related events (e.g., administration of a wrong medication)
- Near miss situations where harm was avoided before reaching the patient
- Adverse events that result in patient harm
- Unplanned events affecting workflow, equipment, or the work environment
- Situations involving risks to both patients and staff
Each of these scenarios is considered reportable and should be documented through an appropriate incident reporting system using a standardized report form.
The Role of the Nurse in Incident Reporting
The nurse plays a central role in writing an incident report, acting as both a frontline observer and a critical contributor to patient safety systems. This responsibility involves:
- Recognizing when an incident has occurred
- Documenting a factual and unbiased account of the incident
- Initiating immediate interventions to stabilize the patient’s condition
- Communicating with the physician, supervisor, and relevant staff
- Ensuring timely submission into the incident reporting system
In high-acuity environments such as the ICU or critical care nursing units, the ability to document events in real time becomes even more essential due to the rapid progression of patient conditions.
The Broader Impact on Patient Safety and Quality Improvement
An Incident Report in Nursing extends beyond individual documentation—it is a critical tool for driving continuous improvement in healthcare systems. Data collected through reporting systems allows organizations to:
- Analyze root causes of incidents
- Develop and implement corrective actions
- Improve workflow efficiency and reduce errors
- Strengthen a positive safety culture
Global health authorities such as the World Health Organization emphasize the importance of structured reporting systems in promoting patient safety and quality improvement. By systematically documenting and reviewing incidents, healthcare systems can move from reactive responses to proactive, preventive strategies.
Ethical and Professional Considerations
When completing an Incident Report in Nursing, adherence to ethical and legal standards is essential:
- Maintain confidentiality in accordance with HIPAA guidelines
- Avoid subjective language—focus strictly on objective facts
- Ensure documentation is concise, accurate, and free from assumptions
- Understand that reports are protected documents but may be reviewed in cases of litigation
Importantly, incident reporting is not intended to be disciplinary but rather a mechanism for improving the quality of care and ensuring safer outcomes for all.
Setting the Stage for Effective Practice
Understanding how to complete an Incident Report in Nursing is a critical competency in modern healthcare practice, particularly within rn health and human services environments and regulated settings such as a nursing facility or those governed by Medicaid policies. Proper documentation ensures that:
- Follow-up actions are clearly defined and implemented
- Communication among healthcare providers is consistent and effective
- Systems are continuously evaluated and improved
This guide builds on these foundational concepts, providing a detailed exploration of how to recognize, document, and manage incidents effectively. By developing strong skills in incident reporting, nurses contribute not only to individual patient outcomes but also to safer, more resilient healthcare systems.
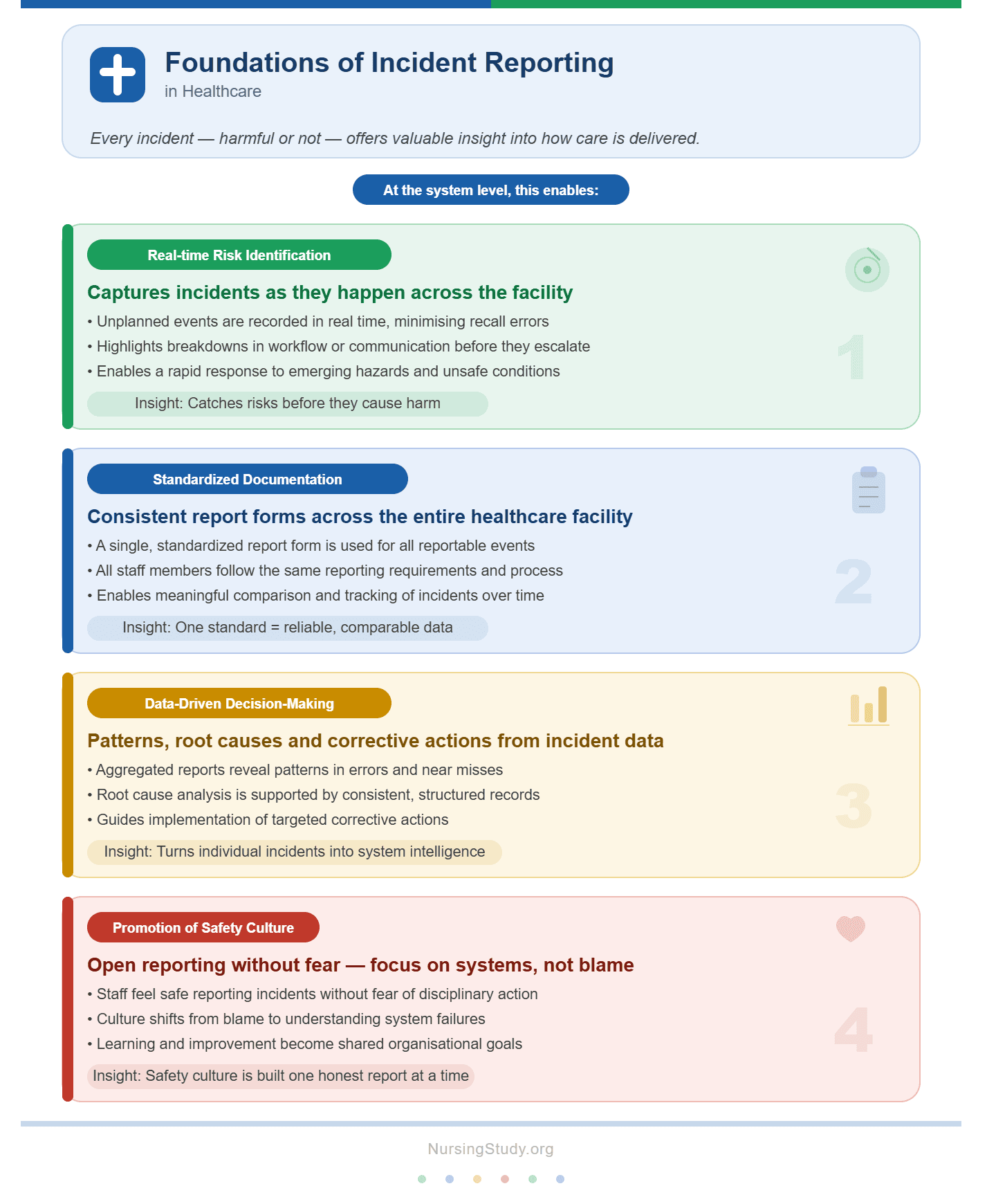
Foundations of Incident Reporting in Healthcare
An Incident Report in Nursing is grounded in the principle that every incident—whether harmful or not—offers valuable insight into how care is delivered within a healthcare setting. In modern healthcare organizations, incident reporting is not an isolated administrative task; it is a structured component of risk management, incident management, and patient safety and quality improvement efforts.
At the system level, an effective incident reporting system enables:
- Real-time identification of risks and hazards
- Captures unplanned events as they occur
- Highlights breakdowns in workflow or communication
- Standardized documentation across the healthcare facility
- Uses a consistent report form for all reportable events
- Ensures all staff members and healthcare professionals follow the same reporting requirements
- Data-driven decision-making
- Allows organizations to identify patterns in errors or near misses
- Supports analysis of root causes and implementation of corrective actions
- Promotion of a safety culture
- Encourages open reporting and learning without fear of disciplinary action
- Focuses on improving systems rather than blaming individuals
Global frameworks, including those promoted by the World Health Organization, emphasize that strong reporting systems are essential for keeping patients safe and improving the overall quality of care. Within health services, especially in regulated environments like a nursing facility or ICU, reporting systems play a central role in ensuring both patients and staff are protected from preventable harm.
The Role of the Nurse in Identifying and Reporting an Incident
The nurse is often the first staff member to observe an incident due to their continuous involvement in patient care. This frontline position places the nurse at the center of writing an incident report and initiating appropriate responses.
Key Responsibilities of the Nurse
- Early Recognition of an Incident
- Identifying deviations from expected care (e.g., incorrect medication, patient fall)
- Recognizing both obvious adverse events and subtle near miss situations
- Immediate Clinical Response
- Implementing necessary interventions to stabilize the patient’s condition
- Notifying the physician and other relevant healthcare providers
- Accurate Documentation
- Recording a clear and factual account of the incident
- Using objective facts rather than opinions or assumptions
- Documenting actions taken and initial patient response
- Timely Reporting
- Submitting the report into the incident reporting system in real time or as soon as possible
- Ensuring compliance with institutional and department of health guidelines
- Collaboration and Communication
- Informing the supervisor and interdisciplinary team
- Participating in follow-up actions and review processes
Example in Practice
- A nurse in a critical care nursing unit administers medication and later realizes the dosage was incorrect.
- Immediate intervention is initiated to monitor and stabilize the patient
- The physician is notified promptly
- The incident report documents the wrong medication dosage, actions taken, and the patient’s response
- The report is submitted through the reporting system for further incident management
In such cases, the nurse’s role is not only clinical but also integral to patient safety and quality improvement across the organization.
Not confident in your nursing writing skills?
We’ll produce clear, professional, and evidence-based work.
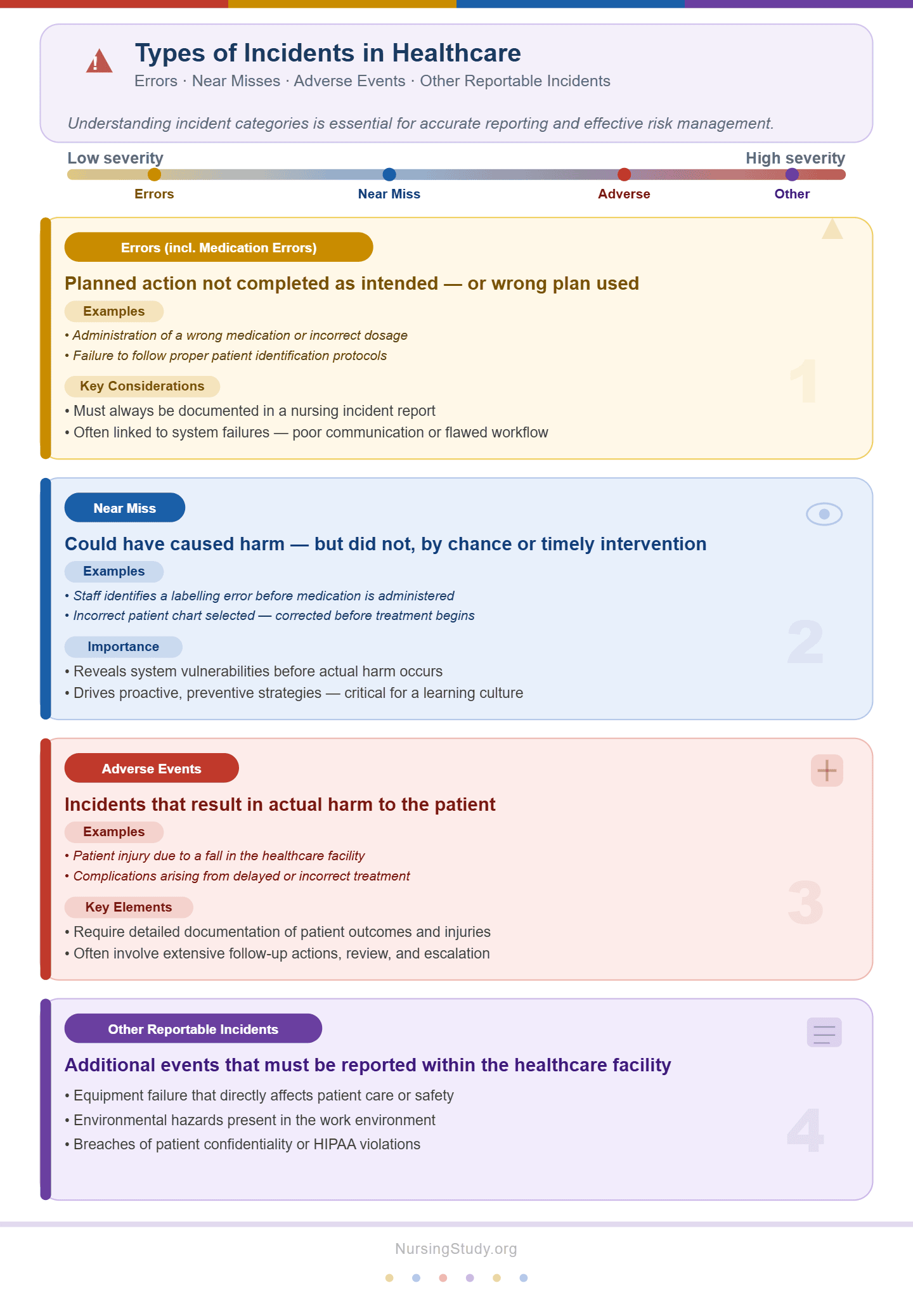
Types of Incidents in Healthcare Settings (Errors, Near Misses, Adverse Events)
Understanding the different types of incident categories is essential for accurate reporting and effective incident management. Each type contributes differently to quality improvement and risk management.
1. Errors (Including Medication Errors)
These occur when a planned action is not completed as intended or the wrong plan is used.
- Example:
- Administration of a wrong medication or incorrect dosage
- Failure to follow proper patient identification protocols
- Key Considerations:
- Must always be documented in an Incident Report in Nursing
- Often linked to system failures such as poor communication or flawed workflow
2. Near Miss
A near miss is an event that could have caused harm but did not, either by chance or timely intervention.
- Example:
- A staff member identifies a labeling error before medication is administered
- Incorrect patient chart selected but corrected before treatment
- Importance:
- Provides critical insight into system vulnerabilities
- Encourages proactive preventive strategies without waiting for harm to occur
3. Adverse Events
These are incidents that result in actual harm to the patient.
- Example:
- Patient injury due to a fall in a healthcare facility
- Complications arising from delayed treatment
- Key Elements:
- Require detailed documentation of patient outcomes
- Often involve more extensive follow-up actions and review
4. Other Reportable Incidents
Additional reportable events may include:
- Equipment failure affecting patient care
- Environmental hazards in the work environment
- Breaches in confidentiality or HIPAA violations
Each category contributes to a broader understanding of risks within healthcare settings, enabling organizations to implement system-wide improvements.
Why Incident Reports Matter for Patient Safety and Quality Improvement
An Incident Report in Nursing is not merely a documentation requirement—it is a cornerstone of patient safety and quality improvement. Its significance extends across clinical, organizational, and legal domains.
1. Enhancing Patient Safety
- Enables rapid response to unplanned events
- Ensures timely intervention and continuity of care
- Helps prevent recurrence of similar incidents
2. Supporting Quality Improvement
- Provides data for analyzing root causes
- Drives continuous improvement initiatives
- Improves the overall quality of care within the healthcare facility
3. Strengthening Risk Management
- Identifies trends and high-risk areas
- Supports proactive corrective actions
- Reduces exposure to legal action and litigation
4. Promoting a Culture of Safety
- Encourages transparency and accountability
- Reduces fear associated with reporting errors
- Builds a positive safety culture among staff and healthcare professionals
5. Ensuring Legal and Regulatory Compliance
- Meets reporting requirements set by health services and regulatory bodies
- Provides legal protection through proper documentation
- Aligns with standards required in settings such as those governed by Medicaid
Example of System Impact
Repeated reports of delayed medication administration in a nursing facility may reveal:
- Staffing shortages
- Inefficient workflow
- Communication gaps among care providers
Through analysis, the organization can implement corrective actions, improving efficiency and ensuring patients safe outcomes.
Principles of Writing an Incident Report in Nursing
An effective Incident Report in Nursing is built on clear principles that prioritize accuracy, accountability, and the protection of both patients and healthcare professionals. Within any healthcare setting, writing an incident report is not simply about completing a report form—it is a structured process that ensures every incident is documented in a way that supports patient safety and quality improvement, strengthens risk management, and contributes to continuous improvement across the system.
At a foundational level, the principles guiding an Incident Report in Nursing include:
- Accuracy and completeness
- Every incident report must reflect what actually occurred without omission
- Details must include time, location, individuals involved (e.g., staff member, physician), and context
- Objectivity and neutrality
- Documentation must rely strictly on objective facts, avoiding assumptions or blame
- The account of the incident should describe events as observed, not interpreted
- Timeliness
- Reporting should occur in real time or as soon as possible after the unplanned event
- Delayed reporting can compromise accuracy and affect patient outcomes
- Confidentiality and professionalism
- All information must be handled in accordance with HIPAA and institutional health services policies
- Only authorized healthcare professionals should access the report
- Clarity and conciseness
- Reports must be concise while still comprehensive
- Avoid unnecessary detail that does not contribute to understanding the incident
These principles ensure that the incident reporting system remains a reliable tool for incident management, enabling organizations to identify patterns, analyze root causes, and implement preventive strategies.
Core Standards for Accurate and Objective Documentation
The quality of an Incident Report in Nursing depends heavily on how well the documentation adheres to established standards. These standards ensure consistency across healthcare organizations and support the broader goals of patient safety and quality.
Key Documentation Standards
- Use of Objective Facts
- Document only what was directly observed or verified
- Avoid subjective language such as “patient appeared careless”
- Example:
- Correct: “Patient found on floor at 10:15 AM beside bed.”
- Incorrect: “Patient fell due to negligence.”
- Clear and Structured Account of the Incident
- Include:
- Date and time of the incident
- Location within the healthcare facility
- Individuals involved (e.g., nurse, staff, physician)
- Sequence of events
- Include:
- Documentation of Actions Taken
- Record all interventions performed immediately after the event
- Include communication with the physician and supervisor
- Note any emergency responses or stabilization measures
- Recording Patient Outcomes
- Document the patient’s condition before and after the incident
- Include any observable changes or complications
- Consistency with the Reporting System
- Ensure all required fields in the report form are completed
- Follow institutional reporting requirements within the incident reporting system
Example of Accurate Documentation
In a critical care nursing environment:
- A nurse administers medication and later identifies a medication error involving a wrong medication.
- The Incident Report in Nursing should include:
- Time and dosage administered
- How the error was identified
- Immediate intervention (e.g., monitoring vital signs)
- Notification of the physician
- Patient’s response and follow-up actions
This structured approach ensures the report contributes meaningfully to incident management and quality improvement.
Legal, Ethical, and Professional Responsibilities of the Nurse
Writing an incident report carries significant legal and ethical implications. The nurse must balance transparency with professional responsibility, ensuring that documentation protects both the patient and the integrity of the healthcare system.
Legal Responsibilities
- Compliance with laws and regulations
- Adhere to guidelines set by the department of health and institutional policies
- Ensure documentation meets standards that may be reviewed in cases of litigation or legal action
- Legal protection through accurate reporting
- A well-documented incident report serves as evidence of appropriate actions taken
- Incomplete or inaccurate reports can increase liability risks
Ethical Responsibilities
- Maintaining confidentiality
- Protect patient information in accordance with HIPAA
- Limit access to authorized healthcare providers only
- Promoting honesty and integrity
- Report all reportable incidents, including near miss events
- Avoid falsification or omission of details
- Supporting a non-punitive safety culture
- Encourage reporting and learning rather than blame
- Contribute to a work environment that prioritizes patients safe outcomes
Professional Responsibilities
- Accountability in patient care
- Recognize and report any hazard or deviation from standard practice
- Ensure timely submission into the reporting system
- Collaboration with the healthcare team
- Communicate with care providers, physician, and supervisor
- Participate in follow-up actions and review processes
- Commitment to quality of care
- Use incident reporting as a tool for improving the quality of care
- Engage in continuous improvement initiatives
Aligning Incident Reporting with Health Services and Regulatory Expectations
An Incident Report in Nursing must align with established health services standards and regulatory frameworks to ensure compliance and effectiveness within the broader healthcare system.
Regulatory Alignment
- Department of Health Requirements
- Many incidents are classified as reportable and must be documented according to national or regional guidelines
- Timelines for submission and escalation must be strictly followed
- Medicaid and Institutional Policies
- Facilities governed by Medicaid often have specific reporting requirements tied to funding and compliance
- Documentation must meet audit and accreditation standards
Organizational Expectations
Within healthcare organizations, incident reporting must support:
- Risk management strategies
- Identifying vulnerabilities in workflow
- Reducing recurrence of adverse events
- Incident management processes
- Coordinating investigation and root causes analysis
- Implementing corrective actions
- Patient safety and quality improvement goals
- Enhancing outcomes across the healthcare facility
- Ensuring safe environments for both patients and staff
Example of Regulatory Alignment in Practice
In a nursing facility, repeated reports of patient falls may trigger:
- Review by a supervisor and safety committee
- Analysis of environmental hazards
- Implementation of preventive measures such as bed alarms or staff training
These actions demonstrate how proper reporting aligns with system-wide efforts to improve safety and compliance.
The Broader Impact
Aligning an Incident Report in Nursing with regulatory and organizational expectations ensures that documentation is not only accurate but also actionable. When consistently applied, these principles:
- Strengthen patient safety and quality improvement initiatives
- Enhance accountability among healthcare professionals
- Support a culture of transparency and excellence in care delivery
Step-by-Step Process of Writing an Incident Report
An Incident Report in Nursing follows a structured, methodical process designed to ensure that every incident is managed safely, documented accurately, and communicated effectively within the healthcare setting. A consistent approach to writing an incident report not only supports immediate clinical care but also strengthens incident management, risk management, and long-term patient safety and quality improvement.
The process can be understood as a sequence of interconnected steps:
- Respond to the incident and ensure patient stability
- Collect and verify accurate information
- Document the event using the appropriate report form
- Submit the report through the incident reporting system
Each step plays a critical role in ensuring that the incident report contributes meaningfully to reporting and learning, supports healthcare organizations, and promotes keeping patients safe.
Immediate Actions Following an Incident in a Healthcare Setting
The first priority in any incident is the safety and well-being of the patient. Before writing an incident report, the nurse must take immediate and appropriate clinical actions.
Key Immediate Actions
- Ensure Patient Safety
- Assess the patient’s condition immediately
- Stabilize the patient using appropriate interventions
- Prevent further harm (e.g., remove environmental hazards)
- Provide Necessary Care
- Initiate emergency protocols if required
- Continue monitoring vital signs, especially in high-risk areas such as the ICU or critical care nursing units
- Notify the Appropriate Personnel
- Inform the physician promptly
- Escalate to the supervisor and other relevant staff members
- Engage additional healthcare providers if needed
- Document Initial Actions in Real Time
- Record immediate observations and actions taken while details are still fresh
- Ensure accuracy by documenting events as they occur in real time
Example Scenario
A patient in a healthcare facility receives a wrong medication:
- The nurse quickly assesses the patient and initiates appropriate intervention
- The physician is notified immediately
- Continuous monitoring is initiated to evaluate patient outcomes
- The situation is stabilized before proceeding to writing an incident report
This step emphasizes that patient care always takes precedence over documentation.
Collecting and Verifying Key Information Before Documentation
Once the patient is stable, the next step in completing an Incident Report in Nursing is gathering accurate and complete information. This ensures the account of the incident is reliable and useful for incident management and quality improvement.
Essential Information to Collect
- Patient Details
- Identification information (without breaching confidentiality)
- Relevant clinical status before the incident
- Incident Details
- Date, time, and exact location within the healthcare setting
- Description of the unplanned event
- Type of event (e.g., medication error, near miss, adverse events)
- People Involved
- Nurse, staff member, or other healthcare professionals present
- Communication with the physician or other care providers
- Actions Taken
- Immediate interventions performed
- Steps taken to mitigate harm
Verification of Information
To maintain objective facts, the nurse should:
- Cross-check details with other staff involved
- Review medication records or equipment logs if applicable
- Avoid assumptions—document only what can be confirmed
Example
In a near miss involving incorrect patient identification:
- The staff member verifies patient details before administering medication
- The error is caught and corrected before harm occurs
- The incident report includes:
- How the error was identified
- Steps taken to prevent administration
- Confirmation from involved healthcare providers
This step ensures the report contributes to identifying root causes and improving systems.
Completing the Incident Report Form in a Nursing Facility
Accurate completion of the report form is central to an effective Incident Report in Nursing. In a nursing facility or other regulated healthcare facility, standardized forms are used to ensure consistency and compliance with reporting requirements.
Key Components of the Report Form
- Basic Information
- Patient details (maintaining confidentiality)
- Date, time, and location of the incident
- Detailed Description
- A clear, chronological account of the incident
- Written using concise and objective language
- Clinical Information
- Patient condition before and after the event
- Any adverse events or complications
- Interventions and Actions Taken
- Immediate care provided
- Communication with the physician and supervisor
- Follow-Up Actions
- Planned monitoring or treatment
- Recommendations for corrective actions
Best Practices for Completing the Report
- Use objective facts only—avoid blame or speculation
- Keep the report concise but comprehensive
- Follow institutional workflow and guidelines
- Ensure all required fields are completed to meet health services and department of health standards
Example
In a fall incident within a nursing facility:
- The incident report includes:
- Exact location (e.g., patient room)
- Time of fall
- Patient’s condition before and after
- Immediate intervention (e.g., assessment, vital signs)
- Notification of the physician and supervisor
This structured documentation supports both immediate care and long-term quality of care improvements.
Submitting the Report to the Incident Reporting System
The final step in the process is submitting the completed incident report into the incident reporting system, ensuring it becomes part of the organization’s official record for analysis and action.
Key Steps in Submission
- Timely Submission
- Reports should be entered into the reporting system as soon as possible
- Delays can affect accuracy and hinder incident management
- Compliance with Reporting Requirements
- Follow institutional, health services, and Medicaid guidelines
- Ensure all reportable incidents are submitted appropriately
- Maintaining Confidentiality
- Protect patient information in accordance with HIPAA
- Limit access to authorized healthcare professionals
Role of the Reporting System
Once submitted, the incident reporting system:
- Aggregates data from multiple reports
- Helps healthcare organizations identify patterns
- Supports analysis of root causes
- Drives system-wide corrective actions and preventive strategies
Example of System Impact
Multiple reports of delayed medication administration across a healthcare facility may reveal:
- Inefficiencies in workflow
- Staffing challenges among staff
- Communication gaps between care providers
Through analysis, leadership can implement targeted improvements, enhancing patient safety and quality improvement.
Importance of Follow-Up
After submission, the process does not end. The nurse and team may be involved in:
- Reviewing the incident with a supervisor
- Participating in follow-up actions
- Contributing to continuous improvement initiatives
Essential Components of an Effective Incident Report
An Incident Report in Nursing is only as strong as the quality and completeness of its documentation. Within any healthcare setting, the purpose of writing an incident report is not merely to record that an incident occurred, but to provide a structured, factual, and clinically meaningful account of the incident that supports incident management, risk management, and long-term patient safety and quality improvement.
A well-constructed report ensures that healthcare professionals, care providers, and healthcare organizations can understand what happened, why it happened, and what actions taken are necessary to prevent recurrence. The essential components below form the foundation of an effective report.
Patient Information and Description of the Incident
The first critical section of an Incident Report in Nursing focuses on identifying the patient and clearly describing the incident as it occurred. This section must be factual, concise, and free from assumptions.
Key Elements to Include
- Patient Information
- Unique identifiers (as permitted under HIPAA and confidentiality rules)
- Clinical context relevant to the patient care situation
- Location within the healthcare facility (e.g., ward, ICU, or critical care nursing unit)
- Description of the Incident
- Date and exact time of the incident
- Clear description of what occurred (e.g., medication error, near miss, or adverse events)
- Sequence of events in chronological order
- Environmental or workflow factors that may have contributed (e.g., hazard, staffing issues among staff members)
Example
A nurse documents:
- “At 10:30 AM, patient in Bed 4 was observed receiving a wrong medication due to mislabeling in the medication tray. The error was identified before full administration.”
This description focuses strictly on objective facts, avoiding judgment or blame.
Interventions, Physician Notification, and Care Provided
Once the incident is identified, immediate clinical response and communication become essential components of the incident report. This section demonstrates how the nurse and healthcare providers responded to ensure patients safe outcomes.
Key Elements to Document
- Immediate Interventions
- First aid or emergency response provided
- Stabilization measures initiated
- Monitoring of vital signs and patient condition
- Physician Notification
- Time the physician was informed
- Instructions received and implemented
- Any changes to treatment plans
- Care Provided
- Ongoing patient care following the incident
- Adjustments to medications or treatment
- Collaboration with other care providers and healthcare professionals
Example
In a near miss involving insulin administration:
- The nurse halts medication delivery immediately
- Blood glucose is checked as an intervention
- The physician is notified and advises continued monitoring
- No harm occurs, but documentation reflects all actions taken
This section is crucial for demonstrating accountability and ensuring continuity of care.
Recording Outcomes and Follow-Up Actions
This section of the Incident Report in Nursing focuses on the patient’s response and the ongoing plan of care after the incident. It also supports broader patient safety and quality improvement efforts.
Key Elements to Include
- Patient Outcomes
- Immediate and delayed response to the incident
- Any changes in clinical condition
- Presence or absence of harm
- Follow-Up Actions
- Monitoring plans established by the healthcare provider team
- Additional tests, treatments, or observations required
- Escalation to higher levels of care if needed
- Preventive Measures
- Steps introduced to prevent recurrence
- Adjustments in workflow or staffing if applicable
- Reinforcement of safety protocols within the healthcare facility
Example
After a patient fall:
- Outcome: Minor bruising, no fractures confirmed
- Follow-up: Neurological checks every 2 hours initiated
- Preventive action: Bed alarm implemented and fall-risk signage added
This documentation supports incident management and helps healthcare organizations improve system safety.
The Role of the Supervisor in Reviewing Incident Reports
The supervisor plays a critical oversight role in ensuring that every Incident Report in Nursing meets institutional and regulatory standards. This review process is essential for maintaining consistency, accountability, and quality of care across the organization.
Key Responsibilities of the Supervisor
- Reviewing Accuracy and Completeness
- Ensuring all sections of the report form are completed
- Verifying that the account of the incident is clear and factual
- Checking that documentation aligns with reporting requirements
- Ensuring Objectivity
- Confirming that the report contains only objective facts
- Removing or addressing subjective or biased language
- Identifying System Issues
- Evaluating whether the incident reflects broader system problems
- Identifying root causes that may require organizational change
- Initiating Corrective Actions
- Recommending corrective actions or preventive measures
- Escalating serious cases to health services, department of health, or regulatory bodies if required
- Supporting Staff Development
- Providing feedback to nurse and staff members on documentation quality
- Reinforcing best practices for writing an incident report
Example of Supervisor Review
A supervisor reviewing multiple incident reports notices repeated medication error patterns in a unit:
- Identifies a breakdown in workflow during medication administration
- Notes staffing shortages among staff members
- Initiates training and system redesign to improve patient safety and quality improvement
This demonstrates how supervisory oversight contributes to incident management and long-term system strengthening.
Incident Reporting Systems and Incident Management
In modern healthcare, an Incident Report in Nursing is not an isolated document but part of a broader digital and organizational structure known as the incident reporting system. This system plays a central role in ensuring that every incident, whether minor or severe, is captured, analyzed, and used to improve safety within the healthcare setting. It is one of the most important tools for strengthening incident management, improving patient safety and quality improvement, and supporting evidence-based decision-making in healthcare organizations.
A well-functioning system ensures that healthcare professionals, including the nurse, physician, and other care providers, can consistently report adverse events, near miss situations, and other reportable occurrences in a structured and standardized way.
Understanding the Incident Reporting System in Healthcare
The incident reporting system is a formal mechanism used by health services and healthcare facilities to document, track, and analyze incidents that affect patient care or staff safety.
Key Features of the Incident Reporting System
- Standardized reporting structure
- Uses a formal report form for consistency
- Ensures all staff members document incidents in a uniform way
- Accessibility for healthcare professionals
- Available to nurse, physician, and other healthcare providers
- Allows reporting across different units such as ICU, wards, and outpatient departments
- Confidential and protected environment
- Maintains confidentiality under HIPAA and institutional policies
- Encourages open reporting and learning without fear of blame
- Real-time reporting capability
- Enables documentation of unplanned events as they occur
- Supports timely escalation of critical incidents
- Integration with organizational systems
- Connects with risk management and quality improvement departments
- Supports compliance with department of health and Medicaid reporting requirements
Example in Practice
In a nursing facility, a patient fall is immediately entered into the incident reporting system by the nurse, including:
- Time and location of the fall
- Patient condition
- Immediate interventions performed
- Notification of the physician and supervisor
This ensures the incident report becomes part of a larger system for review and action.
How Incident Reports Support Incident Management and Risk Reduction
The primary purpose of an Incident Report in Nursing extends beyond documentation. It directly supports incident management and helps reduce risks across the healthcare facility.
Role in Incident Management
Incident management refers to the structured process of identifying, analyzing, and responding to incidents to prevent recurrence.
Incident reports contribute by:
- Identifying what went wrong
- Provides a clear account of the incident
- Captures objective facts for analysis
- Supporting immediate response
- Ensures proper actions taken are documented
- Helps guide ongoing patient care decisions
- Facilitating escalation
- Alerts the supervisor, physician, and relevant healthcare professionals
- Ensures serious events are escalated appropriately
Role in Risk Reduction
Incident reporting is a key component of risk management strategies in healthcare organizations.
It helps to:
- Identify hazards in the work environment
- Detect system weaknesses in workflow
- Prevent recurrence of medication error, wrong medication, or procedural failures
- Reduce exposure to legal action and litigation through proper documentation
Example
A hospital identifies repeated near miss events involving patient identification errors:
- Multiple incident reports highlight scanning failures during medication administration
- Analysis shows inconsistent barcode scanning in a busy unit
- Management introduces corrective training and system updates
This reduces future errors and improves patients safe outcomes.
Using Data from Reporting Systems for Quality Improvement
One of the most powerful functions of the incident reporting system is its ability to generate data that supports quality improvement and system-wide learning.
How Data is Used
- Trend Identification
- Repeated adverse events or near miss patterns are analyzed
- Helps identify patterns across units or departments
- Root Cause Analysis
- Investigates underlying causes of incidents
- Focuses on system failures rather than individual blame
- Performance Monitoring
- Tracks improvements in patient safety and quality over time
- Evaluates effectiveness of corrective actions
- Policy and Workflow Improvement
- Updates clinical guidelines and workflow processes
- Improves coordination among care providers and healthcare professionals
Role in Continuous Improvement
Data from incident reports supports:
- Development of preventive strategies
- Strengthening of safety culture within the organization
- Improvement in overall quality of care
- Reduction in repeat incident occurrences
Example in Practice
A healthcare facility reviews data from its incident reporting system and finds:
- Frequent delays in medication administration during shift changes
- Contributing factors include staffing gaps among staff members and communication breakdowns
As a result, the organization implements:
- Revised handover protocols
- Additional staffing support during peak hours
- Enhanced communication tools for healthcare providers
Over time, incident reports show a decline in medication delays, demonstrating measurable quality improvement.
Reporting Medication Errors and High-Risk Incidents
In any healthcare setting, the accurate handling of medication-related events is a critical aspect of patient safety and quality improvement. An Incident Report in Nursing becomes especially important when dealing with medication error, near miss, and other high-risk incident situations. These events require immediate recognition, precise documentation, and effective communication among healthcare professionals, including the nurse, physician, and other care providers.
Because medication processes involve multiple steps—prescribing, dispensing, administration, and monitoring—there is always potential for breakdowns in workflow, making structured reporting essential for incident management and risk management.
Identifying Medication Errors vs Near Misses
A key competency in writing an incident report is the ability to differentiate between a medication error and a near miss, as both are reportable but have different clinical implications.
Medication Error
A medication error occurs when a patient receives the wrong drug, dose, route, or timing, or when a medication is omitted or duplicated.
Common Examples:
- Administration of a wrong medication
- Incorrect dosage given to a patient
- Failure to administer a prescribed drug
- Incorrect infusion rate in a high-risk medication
Clinical Impact:
- May lead to harm or adverse reactions
- Requires immediate intervention
- Must be documented in an Incident Report in Nursing and escalated to the physician
Near Miss
A near miss is an event that could have caused harm but was prevented before reaching the patient.
Common Examples:
- Wrong medication selected but caught before administration
- Incorrect dose prepared but corrected during verification
- Pharmacy labeling error identified before delivery to the unit
Clinical Importance:
- No patient harm occurs
- Still considered reportable under the incident reporting system
- Valuable for identifying system weaknesses and root causes
Key Distinction
- Medication error → Reaches patient
- Near miss → Prevented before reaching patient
Both require documentation because they contribute to quality improvement and system-wide safety improvements.
Documentation Requirements in Critical Care Nursing
In critical care nursing environments such as the ICU, documentation of medication-related incidents must be especially precise due to the complexity and acuity of patient conditions.
Core Documentation Requirements
An Incident Report in Nursing must include:
- Objective facts only
- Avoid assumptions or blame
- Record exactly what was observed
- Detailed account of the incident
- Time, location, and sequence of events
- Involvement of staff members and healthcare providers
- Medication-specific details
- Name, dose, route, and timing of medication involved
- Clarification of where the breakdown occurred in the process
- Patient condition and outcomes
- Immediate response of the patient’s condition
- Any changes following the incident
- Actions taken
- Emergency interventions initiated
- Monitoring and supportive care provided
- Any corrective steps taken by the nurse
- Use of reporting system
- Entry into the official incident reporting system
- Compliance with reporting requirements and institutional policies
Example in Critical Care
In an ICU setting:
- A patient receives an incorrect infusion rate for a high-alert medication
- The nurse identifies the error during routine monitoring
- Immediate intervention is performed to adjust the infusion
- The event is documented in the report form with:
- Vital signs before and after correction
- Time of discovery and correction
- Notification of the physician
- Follow-up monitoring plan
This ensures accurate incident management and prevents recurrence.
Communicating with the Physician and Healthcare Team
Effective communication is a vital component of managing medication-related incidents. Once a medication error or near miss is identified, timely and structured communication ensures safe continuation of patient care.
Key Communication Responsibilities
1. Immediate Physician Notification
- The physician must be informed promptly after detection
- Communication should include:
- Description of the incident
- Current patient status
- Immediate actions taken
2. Coordination with Healthcare Team
- Inform relevant healthcare professionals involved in care
- Include pharmacy, nursing team, and other care providers when necessary
- Ensure continuity of care across shifts and departments
3. Clear and Structured Reporting
Communication should follow a structured format:
- What happened (brief description of the incident)
- What was done (interventions and corrective steps)
- Current patient condition (patient outcomes)
- What is needed next (orders, monitoring, or escalation)
Example Communication Scenario
A nurse identifies a dosing error in a high-risk medication:
- The physician is immediately notified
- The nurse reports:
- Medication involved
- Time of administration
- Patient’s current vital signs
- Corrective intervention performed
- The healthcare team agrees on increased monitoring and adjustment of treatment
Importance of Team Communication
Effective communication ensures:
- Rapid response to prevent harm
- Coordination among healthcare providers
- Reduction of adverse events
- Strengthening of safety culture in the healthcare facility
Poor communication, on the other hand, can lead to delayed response, worsening patient outcomes, and increased risk of litigation or legal action.
Collaboration and Communication in Incident Reporting
Effective Incident Report in Nursing practice does not occur in isolation. It is deeply dependent on structured collaboration and clear communication among healthcare professionals within a healthcare setting. Because an incident often affects multiple aspects of patient care, coordinated responses from the nurse, physician, care providers, and supervisor are essential for ensuring patient safety and quality improvement.
In modern healthcare organizations, collaboration ensures that an incident reporting system is not just a documentation tool, but a shared mechanism for incident management, risk reduction, and continuous improvement. Without effective communication, even well-documented incident reports may fail to produce meaningful change in outcomes or quality of care.
Working with Physicians, Care Providers, and Supervisors
Collaboration during and after an incident requires coordinated communication between key members of the healthcare team. Each role contributes uniquely to the management and resolution of the event.
Role of the Nurse
The nurse is often the first to identify and respond to an incident. Their responsibilities include:
- Recognizing and initiating immediate intervention
- Documenting a clear, factual account of the incident
- Communicating directly with the physician
- Informing the supervisor and relevant staff members
- Ensuring timely submission into the incident reporting system
Role of the Physician
The physician plays a critical role in clinical decision-making following an incident:
- Evaluates the patient’s condition after the event
- Orders diagnostic tests or treatment adjustments
- Provides clinical direction for ongoing patient care
- Works with the nursing team to prevent further harm
Role of Care Providers
Other care providers, including pharmacists, therapists, and allied health staff, contribute by:
- Reviewing medication or treatment processes
- Supporting monitoring and rehabilitation efforts
- Identifying system-level issues in workflow
- Assisting in implementing corrective actions
Role of the Supervisor
The supervisor ensures that the Incident Report in Nursing process is completed correctly and consistently:
- Reviews the report form for accuracy and completeness
- Ensures compliance with reporting requirements
- Initiates escalation when necessary
- Oversees incident management and follow-up processes
Example Scenario
In a healthcare facility, a patient receives delayed medication due to miscommunication:
- The nurse identifies the delay and documents the incident
- The physician is informed and adjusts the medication schedule
- The supervisor reviews staffing patterns contributing to the issue
- The pharmacy team (care providers) evaluates dispensing workflow
This collaborative approach ensures the incident report leads to meaningful system improvement.
When and How to Escalate an Incident
Escalation is a critical component of incident management, ensuring that high-risk situations receive immediate attention from appropriate leadership and clinical teams.
When to Escalate an Incident
An incident should be escalated when it involves:
- Significant harm or potential harm to the patient
- Serious adverse events or life-threatening conditions
- Repeated medication error patterns
- Failure of initial interventions to stabilize the patient
- System-wide risks affecting multiple staff members or units
How to Escalate an Incident
Escalation should follow a structured process:
- Immediate Notification
- Inform the physician and supervisor without delay
- Activate emergency protocols if required
- Documentation
- Record detailed objective facts in the Incident Report in Nursing
- Include time, actions taken, and patient status
- System Reporting
- Submit the report into the incident reporting system
- Flag the case as urgent or high priority if applicable
- Chain of Communication
- Notify relevant healthcare providers and departments
- Ensure continuity of patient care during transition
Example of Escalation
In an ICU scenario:
- A patient experiences a sudden drop in oxygen saturation due to equipment malfunction
- The nurse initiates immediate intervention and stabilizes the patient
- The physician is urgently called
- The issue is escalated to biomedical engineering and the supervisor
- A formal incident report is submitted for review and investigation
Interdisciplinary Roles in Follow-Up Actions
Follow-up actions after an incident require coordinated efforts across multiple disciplines within the healthcare system. These actions are essential for ensuring that lessons learned translate into continuous improvement and safer care delivery.
Nursing Role in Follow-Up
- Ongoing monitoring of patient outcomes
- Implementation of revised care plans
- Documentation of recovery progress in patient care records
- Participation in debriefing sessions
Physician Role in Follow-Up
- Adjusts treatment plans based on incident findings
- Orders additional diagnostics or interventions
- Evaluates clinical recovery and safety risks
Care Provider Role in Follow-Up
- Reviews contributing system issues (e.g., pharmacy or equipment processes)
- Implements changes to reduce recurrence of hazards
- Supports rehabilitation and recovery services
Supervisor and Organizational Role
- Leads incident management reviews
- Conducts root cause analysis to identify system-wide failures
- Implements corrective actions and preventive strategies
- Ensures compliance with health services and regulatory standards
Example of Interdisciplinary Follow-Up
After a repeated near miss involving incorrect medication labeling:
- Nursing staff adjust verification procedures
- Pharmacy improves labeling protocols
- The supervisor implements double-check systems
- Training sessions are introduced for all staff members
This coordinated response strengthens patient safety and quality improvement across the facility.
Regulatory and Organizational Requirements in Incident Reporting
An Incident Report in Nursing is not only a clinical and safety tool but also a regulated documentation process governed by strict organizational and legal frameworks. Within any healthcare setting, writing an incident report must align with institutional policies, national health services standards, and external regulatory expectations. These requirements ensure that every incident is documented consistently, reviewed appropriately, and used to improve patient safety and quality improvement across healthcare organizations.
Failure to comply with these requirements can lead to gaps in incident management, compromised patient care, and increased risk of legal action or litigation for both individuals and institutions.
Compliance with Health Services and Healthcare Policies
Compliance is a foundational principle of effective Incident Report in Nursing practice. Every healthcare facility operates under established health services policies that define how reportable events must be documented and managed.
Key Compliance Requirements
- Adherence to Institutional Policies
- All staff members, including the nurse, must follow standardized procedures for writing an incident report
- Use of approved report form formats within the incident reporting system
- Ensuring consistency across all departments, including ICU and critical care nursing units
- Timely Reporting
- Incidents must be documented in real time or within a defined timeframe
- Delays may compromise incident management and patient safety and quality outcomes
- Confidentiality Standards
- Compliance with HIPAA and privacy regulations
- Protection of patient’s personal and clinical information
- Restricted access to authorized healthcare professionals only
- Accuracy and Objectivity
- Reports must be based on objective facts
- Avoid subjective interpretation or blame assignment
Example in Practice
In a hospital unit, a medication error occurs during shift change:
- The nurse documents the incident immediately
- The report follows institutional health services guidelines
- The supervisor reviews it for compliance and completeness
- The case is submitted through the official incident reporting system
This ensures alignment with organizational policy and supports risk management.
The Role of Medicaid and Institutional Reporting Guidelines
Regulatory frameworks such as Medicaid and internal institutional guidelines play a significant role in shaping how an Incident Report in Nursing is completed and utilized.
Role of Medicaid Requirements
In facilities funded or regulated under Medicaid, reporting standards are particularly strict:
- Mandatory documentation of adverse events and serious incidents
- Reporting timelines that must be strictly followed
- Documentation audits to ensure compliance with care standards
- Emphasis on protecting patients safe outcomes in long-term care settings
Non-compliance may affect funding, accreditation, and organizational credibility.
Institutional Reporting Guidelines
Each healthcare organization develops its own internal policies based on national standards and regulatory frameworks.
These guidelines typically define:
- What constitutes a reportable incident
- Required steps for incident management
- Roles of healthcare providers, physician, and care providers
- Escalation procedures for high-risk events
- Documentation expectations for patient care continuity
Example Scenario
In a nursing facility:
- A patient fall is classified as a reportable event under institutional policy
- The nurse completes the incident report using the approved system
- The supervisor ensures compliance with Medicaid documentation standards
- Data is later used for facility-wide quality improvement initiatives
Documentation Standards in a Nursing Facility
Accurate and standardized documentation is essential in ensuring that an Incident Report in Nursing meets both clinical and regulatory expectations, particularly in a nursing facility where vulnerable populations require consistent oversight.
Core Documentation Standards
- Structured Reporting Format
- Use of standardized report form templates
- Consistent fields for time, location, individuals involved, and description of the incident
- Objective and Factual Language
- Documentation must reflect objective facts only
- Avoid assumptions about cause or responsibility
- Example:
- Correct: “Patient found on floor at 08:15 AM”
- Incorrect: “Patient fell due to negligence”
- Comprehensive Incident Description
- Clear account of the incident including sequence of events
- Identification of contributing hazards or workflow issues
- Inclusion of Clinical Details
- Interventions performed by the nurse
- Notification of the physician and response from healthcare providers
- Documentation of patient outcomes
- Follow-Up Documentation
- Recording actions taken after the event
- Noting corrective actions and preventive strategies
- Updating ongoing patient care plans
Example in a Nursing Facility
A resident in a nursing facility experiences a medication delay:
- The nurse documents the delay with exact timing and medication details
- The physician is informed and adjusts the treatment plan
- The supervisor reviews staffing-related workflow issues
- The report contributes to a broader review of incident management processes
The Role of Incident Reporting in Patient Safety and Quality Improvement
An Incident Report in Nursing is a central mechanism through which healthcare organizations strengthen patient safety and quality improvement. Rather than functioning as a routine administrative task, the process of writing an incident report transforms individual incident occurrences into structured learning opportunities that improve patient care, reduce risks, and enhance system performance across the healthcare setting.
In practice, every documented incident—whether a medication error, near miss, or adverse events—contributes to a broader understanding of how care processes function in real-world environments such as the ICU, general wards, or a healthcare facility. When effectively utilized, incident reporting systems become powerful tools for identifying weaknesses in workflow, strengthening incident management, and improving outcomes for both patients and staff.
Linking Incident Reports to System-Level Improvements
One of the most important roles of an Incident Report in Nursing is its contribution to system-wide analysis and improvement. Instead of focusing solely on individual mistakes, modern healthcare organizations use incident data to identify patterns and correct underlying system failures.
How Incident Reports Drive System-Level Change
- Identification of Root Causes
- Repeated incident documentation helps uncover systemic issues rather than isolated errors
- Focus is placed on root causes such as communication breakdowns, staffing challenges, or equipment failures
- Detection of Patterns
- Aggregated reports allow organizations to identify patterns in adverse events or near miss situations
- Example: repeated delays in medication administration during shift changes
- Workflow Optimization
- Analysis of reports reveals inefficiencies in workflow processes
- Improvements are made to reduce delays, duplication, or miscommunication among care providers
- Corrective and Preventive Actions
- Implementation of corrective actions based on findings
- Development of preventive strategies to reduce recurrence of similar incidents
Example
A hospital notices multiple incident reports involving incorrect patient identification before medication administration:
- Investigation reveals inconsistent scanning procedures
- A system-wide update introduces mandatory barcode verification
- Additional staff training is conducted for all healthcare professionals
This demonstrates how Incident Report in Nursing contributes directly to safer, more efficient systems.
Building a Culture of Safety in Healthcare
A strong safety culture is essential for effective patient safety and quality improvement. Incident reporting plays a foundational role in shaping this culture by encouraging transparency, accountability, and continuous learning within the healthcare system.
Key Elements of a Safety Culture
- Non-punitive reporting environment
- Encourages reporting and learning rather than blame
- Reduces fear of disciplinary action among staff members
- Transparency in communication
- Open sharing of incident reports among healthcare providers
- Honest documentation of objective facts
- Continuous learning and improvement
- Every incident is treated as a learning opportunity
- Emphasis on system improvement rather than individual fault
- Leadership support
- Supervisors and administrators actively support reporting practices
- Commitment to improving quality of care across all units
Example
In a nursing facility, staff are encouraged to report near miss events involving medication administration:
- Nurses report errors without fear of punishment
- Management reviews reports to improve training programs
- Communication between shifts is strengthened
Over time, this builds trust and improves patients safe outcomes.
The Contribution of Student Nurses to Quality Improvement Initiatives
Although often in training roles, student nurses play an important part in supporting patient safety and quality improvement through participation in Incident Report in Nursing processes. Their involvement helps build foundational skills in writing an incident report and understanding incident management within real clinical environments.
Roles of Student Nurses in Incident Reporting
- Observation and early identification
- Recognizing incident situations such as near miss events or workflow errors
- Reporting observations to supervising nurse or physician
- Assisting in documentation
- Learning how to complete a report form accurately under supervision
- Understanding how to document objective facts clearly and concise
- Participation in feedback and learning sessions
- Engaging in post-incident reviews led by supervisors
- Learning from root causes and corrective actions discussions
- Supporting safe care practices
- Applying lessons learned to improve future patient care
- Contributing to a culture of keeping patients safe
Example
A student nurse observes a delay in administering antibiotics due to miscommunication during shift handover:
- Reports the issue to the supervising nurse
- Assists in documenting the incident report
- Participates in a review meeting discussing workflow improvements
- Learns how communication breakdowns affect patient outcomes
This experience reinforces the importance of structured reporting in real clinical practice.
Challenges and Best Practices in Incident Reporting
An Incident Report in Nursing is a critical tool for strengthening patient safety and quality improvement, yet its effectiveness depends heavily on how consistently and accurately healthcare professionals engage in writing an incident report. In real-world healthcare settings, multiple barriers can limit proper documentation of an incident, affecting incident management, risk management, and overall quality of care.
Understanding these challenges—and applying effective best practices—ensures that every incident report contributes meaningfully to safer systems, improved patient care, and stronger healthcare organizations.
Common Barriers in Reporting Incidents in Healthcare
Despite clear policies within most healthcare facilities, several barriers continue to affect the quality and frequency of reporting through the incident reporting system.
1. Heavy Workload and Time Constraints
- High patient-to-nurse ratios limit time for documentation
- Prioritization of urgent patient care over reporting
- Delays in completing the report form, reducing accuracy
2. Lack of Awareness or Training
- Some staff members may not fully understand what constitutes a reportable incident
- Confusion between near miss, adverse events, and minor errors
- Inconsistent knowledge of reporting requirements across departments
3. Complex Reporting Systems
- Difficult or time-consuming digital incident reporting system interfaces
- Lack of integration with daily workflow
- Technical challenges in submitting reports in real time
4. Fear of Consequences
- Concern about disciplinary action
- Fear of negative evaluation from supervisors
- Anxiety about potential legal action or litigation
5. Poor Communication Structures
- Limited feedback after submitting an incident report
- Weak communication between healthcare providers, physicians, and care providers
- Lack of clarity on follow-up actions
Example
In a busy ICU, a nurse notices a delayed medication administration but fails to document it due to workload pressure and uncertainty about whether it qualifies as a reportable event. As a result, a potential system issue in workflow remains unaddressed.
Overcoming Fear, Blame Culture, and Underreporting
One of the most significant barriers to effective Incident Report in Nursing practice is the presence of a blame-oriented culture. This often leads to underreporting, which undermines incident management and weakens patient safety and quality improvement systems.
1. Shifting from Blame to Learning
Modern healthcare organizations promote a safety culture where the focus is on:
- Identifying root causes instead of individual fault
- Encouraging reporting and learning
- Treating each incident as an opportunity for system improvement
2. Reducing Fear of Reporting
To overcome fear among healthcare professionals:
- Ensure confidentiality of the incident reporting system
- Emphasize HIPAA compliance and protection from misuse of reports
- Reinforce that reporting is not intended for punishment but improvement
3. Addressing Underreporting
Underreporting weakens data used for quality improvement. Solutions include:
- Regular training for staff members on identifying near miss and adverse events
- Encouraging leadership support from supervisors and administrators
- Providing feedback after submission of an Incident Report in Nursing
Example
A hospital introduces anonymous reporting for near miss medication events. Over time:
- Reporting rates increase significantly
- Previously hidden patterns of medication error are identified
- System changes reduce recurrence of errors
This demonstrates how reducing fear improves incident management outcomes.
Best Practices for Accurate and Timely Incident Documentation
Effective writing an incident report requires consistency, clarity, and adherence to structured documentation principles. Best practices ensure that every incident report contributes to safer healthcare settings and better decision-making.
1. Timely Documentation
- Report the incident as soon as possible after it occurs
- Ensure real time accuracy of events
- Avoid delays that may compromise memory or detail accuracy
2. Use Objective and Concise Language
- Document only objective facts
- Avoid assumptions or emotional language
- Keep descriptions concise and structured
Example:
- Correct: “Patient found on floor at 07:45 AM near bedside.”
- Incorrect: “Patient fell because staff were careless.”
3. Complete All Required Sections
- Ensure full completion of the report form
- Include details of:
- Patient’s condition
- Actions taken
- Interventions provided
- Notification of physician and supervisor
4. Ensure Clear Communication
- Clearly document communication with healthcare providers
- Include instructions given by the physician
- Record follow-up actions and monitoring plans
5. Maintain Confidentiality and Compliance
- Follow HIPAA guidelines
- Protect sensitive patient care information
- Ensure compliance with department of health and institutional policies
6. Support Continuous Improvement
- Highlight contributing factors such as workflow issues or staffing challenges
- Help organizations identify patterns in recurring incidents
- Contribute to corrective actions and preventive strategies
Example
In a nursing facility, a fall incident is reported:
- The nurse documents time, location, and patient condition
- Immediate intervention is recorded
- The physician is notified and follow-up monitoring is initiated
- The supervisor later reviews the report and identifies poor lighting as a contributing hazard
This leads to environmental improvements across the facility.
Practical Tips for Student Nurses Writing Incident Reports
An Incident Report in Nursing is a core component of safe and effective patient care in any healthcare setting. While structured guidelines exist, the ability to apply them correctly in real clinical environments depends on practice, attention to detail, and understanding how healthcare professionals use documentation to support incident management and patient safety and quality improvement.
For those learning writing an incident report, developing strong documentation habits early is essential because it directly influences healthcare outcomes, legal protection, and organizational risk management within healthcare organizations.
Avoiding Common Documentation Mistakes
One of the most important skills in writing an incident report is recognizing and avoiding common documentation errors that can compromise clarity, accuracy, or legal defensibility.
1. Including Opinions Instead of Objective Facts
- A frequent mistake is inserting personal judgment instead of objective facts
- Incident reports must describe what happened, not why it happened unless confirmed
Example:
- Incorrect: “The nurse was careless and caused the error.”
- Correct: “Medication was administered at the incorrect time as documented in the chart.”
2. Incomplete Descriptions of the Incident
- Failing to provide a full account of the incident reduces the usefulness of the report in incident management
- Missing details such as time, location, or patient’s condition can affect analysis
3. Delayed Reporting
- Waiting too long after an incident can result in forgotten details
- Real time reporting improves accuracy and supports faster intervention
4. Omitting Actions Taken
- Not documenting actions taken or interventions can create gaps in continuity of patient care
- It also weakens the effectiveness of the incident reporting system
5. Breaching Confidentiality
- Including unnecessary identifiers violates HIPAA and institutional health services policies
- Only essential patient information should be recorded
Example
A student nurse documents a fall but forgets to include:
- Time of the incident
- Immediate response by the nurse
- Notification of the physician
This incomplete documentation limits the ability of the supervisor and care providers to conduct proper incident management review.
Writing Clear, Concise, and Objective Reports
Clarity and precision are essential in an Incident Report in Nursing. Reports should be structured so that any healthcare provider can quickly understand what occurred and what actions were taken.
1. Use Clear and Simple Language
- Avoid complex or emotional wording
- Stick to factual descriptions of the incident
2. Be Concise but Complete
- Include all relevant details without unnecessary elaboration
- Focus on key elements:
- What happened
- When and where it occurred
- Who was involved (staff members, physician, etc.)
- What was done
3. Maintain Objectivity
- Only document what was observed or verified
- Avoid assumptions about root causes unless confirmed through investigation
4. Use Chronological Order
- Present events in sequence to improve understanding of the incident
- Helps healthcare organizations analyze workflow breakdowns effectively
Example
Instead of writing:
“The patient became very upset and the nurse probably made a mistake which caused confusion.”
A clear, objective report would state:
“At 14:20, patient was found confused after receiving medication. The nurse reviewed the medication chart and identified a timing discrepancy. The physician was notified, and monitoring was initiated.”
5. Focus on Clinical Relevance
- Include only information relevant to patient safety and quality improvement
- Avoid irrelevant personal observations
Preparing for Real-World Incident Reporting in Clinical Practice
Transitioning from training to real clinical environments requires confidence in writing an incident report and understanding how it functions within broader healthcare systems.
1. Understanding Reporting Systems Early
- Familiarize yourself with the incident reporting system used in the clinical site
- Learn how to access and complete the report form
- Understand reporting requirements for different types of incidents
2. Observing Experienced Healthcare Professionals
- Watch how experienced nurses, physicians, and care providers respond to incidents
- Pay attention to communication patterns and documentation practices
3. Practicing Clinical Judgment
- Learn to identify:
- Near miss situations
- Adverse events
- Medication-related errors
- Understand what is considered reportable
4. Developing Communication Skills
- Practice clear reporting to supervisors and healthcare teams
- Learn structured communication when escalating an incident
- Ensure timely notification of the physician when needed
5. Embracing a Safety Culture
- View reporting as part of patient safety and quality improvement, not punishment
- Understand that every incident report contributes to safer systems
- Participate in discussions on corrective actions and improvements in workflow
Example
During clinical placement in a healthcare facility, a student nurse observes a near miss where a patient almost receives the wrong medication:
- The student reports the observation to the supervising nurse
- Assists in completing the incident report
- Learns how the supervisor uses the report to identify a labeling issue in pharmacy processes
- Sees how the event leads to improved safety protocols
Not confident in your nursing writing skills?
We’ll produce clear, professional, and evidence-based work.
Conclusion
An Incident Report in Nursing is more than a documentation requirement within a healthcare setting; it is a fundamental mechanism for strengthening patient safety and quality improvement across all levels of care. Every incident, whether a medication error, near miss, or adverse events, represents a critical learning opportunity that contributes to improved patient care, safer healthcare systems, and more effective incident management practices within healthcare organizations.
When properly executed, writing an incident report ensures that objective facts are accurately captured, allowing healthcare professionals—including the nurse, physician, and other care providers—to understand what occurred, what actions taken were implemented, and what further corrective actions are needed. This structured approach supports the incident reporting system, enabling organizations to identify patterns, analyze root causes, and implement preventive strategies that reduce future risk.
Equally important, effective incident reporting strengthens a culture of transparency and accountability. In environments where health services emphasize learning over blame, staff members are more likely to engage in reporting and learning, contributing to a stronger safety culture. This shift is essential in reducing underreporting, improving communication, and ensuring that both patients and staff are protected from avoidable harm.
For those entering clinical practice, particularly within critical care nursing, mastering the principles of Incident Report in Nursing builds a foundation for professional responsibility and ethical practice. It reinforces the importance of timely documentation, clear communication with the supervisor and physician, and adherence to regulatory expectations such as reporting requirements, HIPAA, and institutional guidelines.
Ultimately, effective incident reporting transforms individual experiences into system-wide improvements. It ensures that every incident contributes to safer healthcare facilities, improved workflow, and stronger outcomes in patient safety and quality improvement. By embracing this responsibility, nurses and other healthcare professionals actively contribute to a more resilient, responsive, and continuously improving healthcare system.
Frequently Asked Questions
How to write an incident report for a nurse?
To write an incident report in nursing, the nurse should:
- Ensure patient safety first by providing or assisting with immediate care
- Document the event as soon as possible (real time or shortly after)
- Record only objective facts (what was seen, heard, or done)
- Include key details: time, location, patient’s condition, and individuals involved
- Describe actions taken, including any intervention and notification of the physician or supervisor
- Submit the report using the facility’s official incident reporting system
How do you write an incident report example?
An example of writing an incident report in nursing should follow a clear structure:
- What happened: Patient found on floor at 08:10 AM
- Where and when: Ward room, morning shift
- Who was involved: Patient and assigned nurse
- What was done: Patient assessed, vital signs taken, physician notified
- Outcome: No fractures identified, monitoring initiated
The report should be concise, factual, and free from opinion.
What are the 6 examples of situations in which you should complete an incident report?
An incident report should be completed in situations such as:
- Medication error (e.g., wrong drug or dose)
- Patient fall or injury
- Near miss (error caught before reaching patient)
- Equipment or device failure affecting care
- Adverse events during treatment or procedures
- Breach of patient safety protocols or identification errors
What are the 5 elements of a good incident report?
A good incident report in nursing includes:
- Accurate patient and incident details (time, place, description)
- Objective facts only (no opinions or blame)
- Clear description of actions taken and interventions
- Documentation of communication (e.g., notification of physician/supervisor)
- Patient outcomes and follow-up actions
These elements ensure the report supports patient safety and quality improvement and effective incident management.