
Jackknife Position in Surgical Practice: Prone Position, Anorectal Surgery, Anesthesia, Spinal Patient Positioning, and Intraoperative Hemodynamics in Ambulatory and Kraske Procedures
The operating room represents one of the most structured environments in clinical practice, where patient outcomes depend on precise coordination between positioning, anesthesia, and surgical planning. Within this setting, the Jackknife Position holds a specialized role in colorectal and anorectal surgery because it enhances exposure of deep pelvic structures while supporting operative precision and safety. In perioperative care, position is not a passive step but a deliberate clinical intervention that influences airway patency, circulation, tissue perfusion, and surgical access. The Jackknife Position is a modified form of the prone position, in which the body is flexed at the abdomen while the hips are elevated, creating a V-shaped configuration that improves visualization of the posterior pelvic region. In this configuration, the prone jackknife position is widely applied in anorectal interventions where access to the rectum and anus is essential for safe and effective execution of a surgical procedure.
Foundations of the Jackknife Position and Prone Position in Surgical Practice
The Jackknife Position and the prone position are foundational concepts in perioperative and surgical care because they directly determine exposure, accessibility, and physiological stability during a wide range of procedures. In operative environments, position during surgery is not a secondary consideration; it is a core determinant of surgical success, influencing both the ease of the surgical procedure and the safety of the patient position. This is particularly evident in anorectal surgeries, where deep pelvic access is required and even small variations in positioning can significantly affect surgical visibility and outcomes.
Definition and clinical characteristics of the jackknife position and prone position
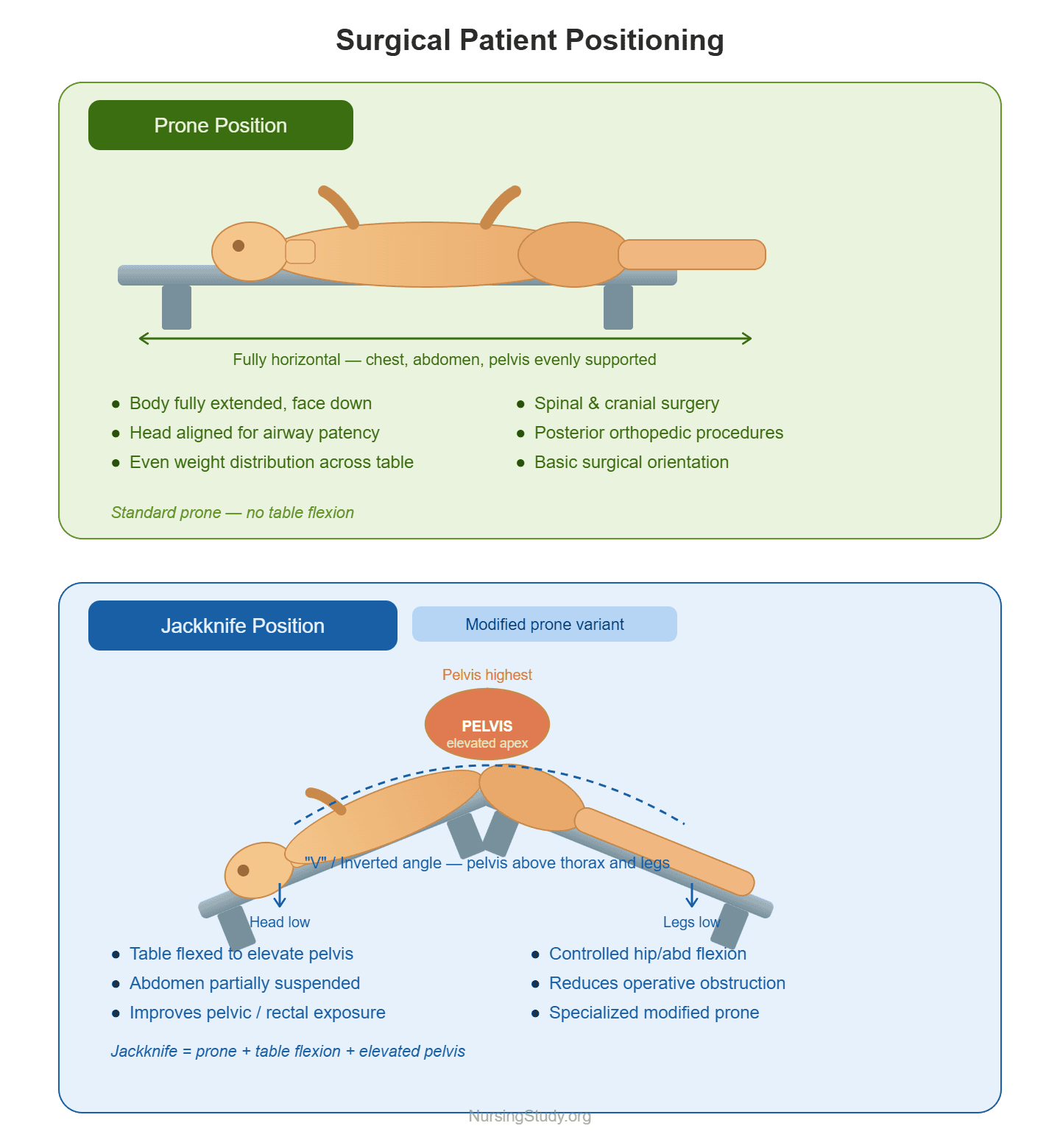
The prone position refers to a basic surgical orientation in which the patient lies face down on the operating surface. In this configuration:
- The body is fully extended in a horizontal alignment
- The chest, abdomen, and pelvis are supported evenly
- The head and neck are aligned to maintain airway patency
- It is commonly used in spinal surgery, posterior cranial procedures, and certain orthopedic interventions
In contrast, the Jackknife Position is a modified and more specialized variant of the prone setup. It is designed to improve pelvic exposure by introducing controlled flexion at the abdominal and hip regions. Key clinical characteristics include:
- The patient is placed in a prone orientation
- The operating table is flexed to elevate the pelvis above the thorax
- The body forms a “V” or inverted angle
- The head and legs are positioned lower relative to the pelvis
- The abdomen is partially suspended to reduce obstruction of the operative field
This configuration is frequently used in anorectal procedures, where direct access to the rectum and anus is required. The design of the Jackknife Position ensures that gravity assists in moving abdominal contents away from the pelvis, improving surgical visualization and precision.
Differences between prone position and jack knife position in surgical practice
Although the prone position and jack knife position share a similar base orientation, their functional applications differ significantly in surgical practice.
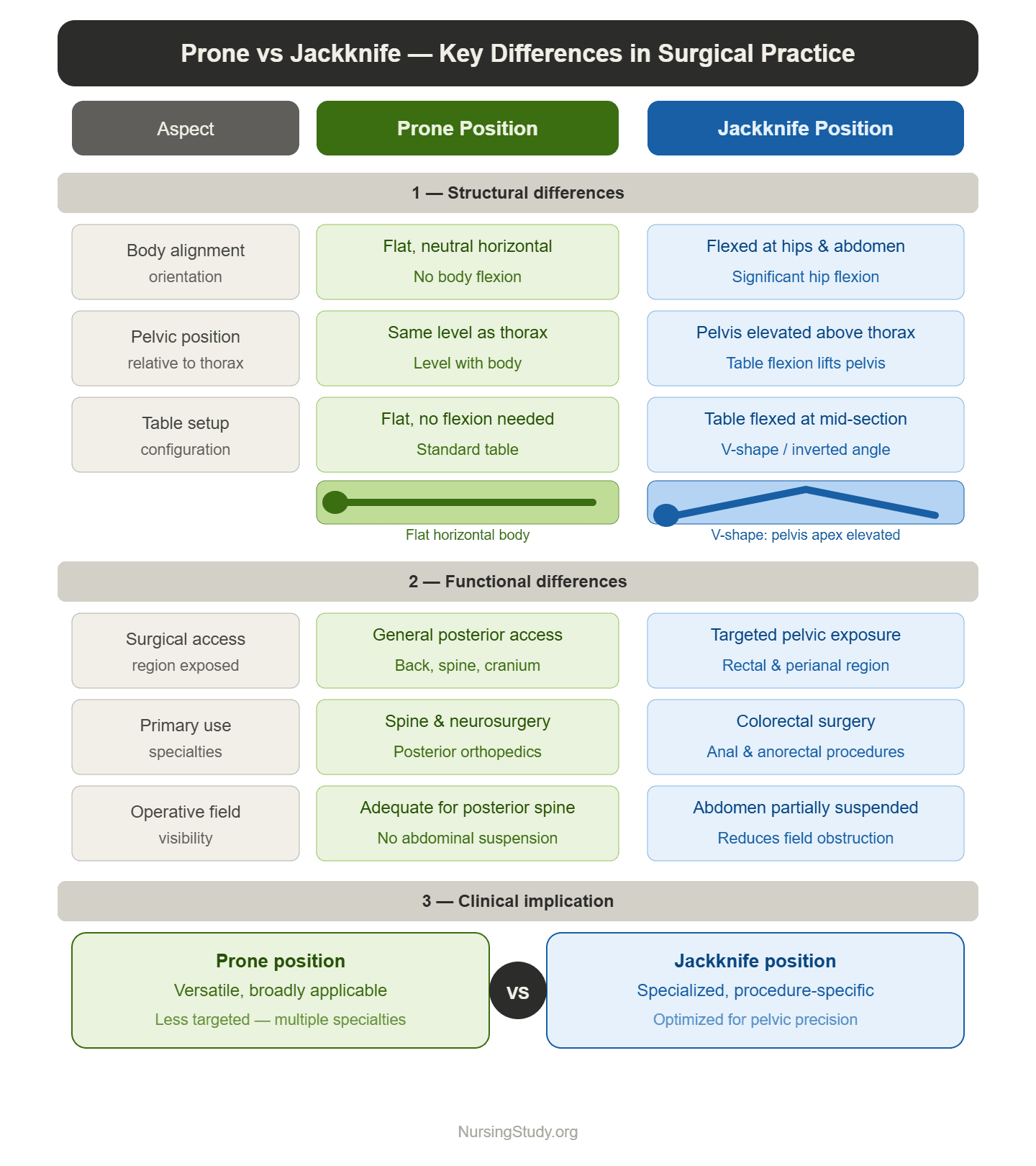
1. Structural differences
- Prone position
- Flat, neutral alignment of the body
- Minimal or no flexion at the hips
- Broadly used across multiple specialties
- Jackknife Position
- Significant flexion at the hips and abdomen
- Elevation of pelvic region using operating table adjustments
- Designed specifically for pelvic and anorectal access
2. Functional differences
- Prone position:
- Provides general posterior access
- Common in spine surgery and neurosurgical procedures
- Jackknife Position:
- Optimizes exposure of the rectal and perianal region
- Enhances precision in colorectal surgeries and anal procedures
3. Clinical implication
- The prone position is versatile but less targeted
- The Jackknife Position is specialized and procedure-specific
For example, a patient undergoing lumbar spinal decompression would be placed in a prone position, whereas a patient undergoing hemorrhoidectomy would require the prone jackknife position for optimal exposure.
Behind on multiple nursing assignments?
Our team will handle them while you focus on learning and clinical work.
Surgical significance of the prone jackknife position in anorectal and perianal procedures
The prone jackknife position holds major clinical importance in anorectal surgeries and perianal interventions due to its ability to enhance surgical access and precision.
Key surgical advantages include:
1. Improved anatomical exposure
- Direct visualization of the anus, rectum, and perianal structures
- Reduced obstruction from abdominal organs
- Enhanced access during delicate dissection
2. Enhanced surgical efficiency
- Shorter operative time due to improved exposure
- Reduced need for excessive retraction
- Better instrument maneuverability during operative procedures
3. Common clinical applications
The position is frequently used in:
- Hemorrhoidectomy
- Anal fistula repair
- Perianal abscess drainage
- Complex anorectal procedures involving tissue excision or reconstruction
For example, during a fistula-in-ano repair, the Jackknife Position allows the surgical team to clearly visualize the tract and surrounding tissue, improving precision and reducing the risk of incomplete excision.
4. Physiological benefit to surgical access
The flexed configuration improves gravitational displacement of abdominal structures, making it easier to access deep pelvic tissues without excessive manipulation.
Kraske position and historical development of jackknife positioning techniques
The kraske position, also known as the Kraske position, represents the historical foundation from which modern jackknife techniques evolved. It was initially developed to improve access to the posterior pelvic cavity during rectal surgery.
1. Historical origins
- Introduced in the late 19th century for improved rectal access
- Designed to address limitations of earlier supine and lithotomy approaches
- Focused on improving exposure of the lower rectum
2. Key characteristics of the Kraske position
- Patient positioned prone
- Pelvis elevated using bolsters or supports
- Abdomen allowed to hang freely to reduce pressure
- Enhanced exposure of deep pelvic structures
3. Evolution into the modern Jackknife Position
Over time, the Kraske position was refined into what is now known as the Jackknife Position, with improvements including:
- Adjustable surgical tables replacing manual supports
- Better pressure-relieving padding systems
- Improved anesthetic monitoring during positioning
- Safer control of hemodynamics during prolonged procedures
4. Clinical relevance today
Modern surgical practice still draws from the Kraske concept, particularly in:
- Complex colorectal surgeries
- Abdominoperineal resection procedures
- Advanced anorectal surgical procedures involving deep pelvic access
For example, in rectal cancer surgery requiring abdominoperineal resection, the evolution of jackknife positioning allows for safer and more controlled access compared to earlier historical techniques.
Clinical Applications of Jackknife Position During Surgery
The Jackknife Position is a highly specialized form of surgical positioning that plays a central role in lower gastrointestinal procedures, particularly where deep pelvic exposure is required. In clinical practice, the effectiveness of a surgical procedure is closely linked to how well the patient position supports access to the surgical site, minimizes intraoperative complications, and maintains physiological stability. The prone jackknife position is therefore widely used in anorectal, colorectal, and anal surgery due to its ability to improve visualization, reduce obstruction, and enhance precision during operative intervention.
Use of jackknife position in anorectal, colorectal, and anal surgical procedures
The Jackknife Position is most commonly associated with procedures involving the distal gastrointestinal tract, where access to the rectum and anus is essential.
1. Anorectal surgical applications
In anorectal surgeries, the position is used to optimize exposure of superficial and deep perianal structures. Common procedures include:
- Hemorrhoidectomy
- Fistula-in-ano repair
- Incision and drainage of perianal abscesses
- Excision of anal fissures
In these cases, the patient is placed in a prone orientation with controlled flexion to ensure that the anal canal is directly accessible. The Jackknife Position allows gravitational separation of soft tissues, reducing the need for excessive retraction and improving surgical precision.
2. Colorectal surgical applications
In colorectal surgeries, particularly those involving the distal colon and rectum, the position enhances operative access by:
- Improving visualization of the rectal vault
- Allowing deeper pelvic dissection
- Facilitating precise tissue removal during resection procedures
For example, during low anterior resection for rectal lesions, the prone jackknife position provides improved alignment for dissection and stapling techniques.
3. Anal surgical applications
In anal procedures, the position is particularly valuable because:
- It exposes the anal sphincter complex clearly
- It improves access for minimally invasive interventions
- It allows for accurate identification of pathology
Overall, the position during surgery significantly enhances procedural accuracy in anorectal and anal interventions.
Ambulatory anorectal surgery and patient positioning strategies
In modern healthcare systems, many anorectal procedures are performed in outpatient or short-stay settings under ambulatory surgery models. In this context, the Jackknife Position is particularly advantageous due to its efficiency and ability to optimize surgical exposure while minimizing recovery time.
Key positioning strategies in ambulatory settings include:
- Preoperative planning of patient position
- Assessment of patient anatomy and surgical target
- Determination of whether prone jackknife positioning is required
- Efficient transition into surgical position
- The patient is placed in a prone position after anesthesia induction
- Controlled elevation of the pelvis using the operating table
- Optimization of surgical workflow
- Reduced repositioning during the procedure
- Faster setup compared to more complex positioning systems
- Postoperative recovery considerations
- Minimization of prolonged compression
- Early mobilization after postoperative stabilization
For example, in outpatient hemorrhoidectomy, the Jackknife Position allows rapid access and efficient completion of the procedure, reducing overall operating time and improving turnover in ambulatory surgical units.
Comparison of prone jackknife position with lateral and alternative surgical positions
Different surgical positioning techniques are used depending on the anatomical target, surgical complexity, and anesthetic requirements. The prone jackknife position must be understood in relation to alternative positions such as the lateral position, supine position, and other modified approaches.
1. Prone jackknife position
- Provides maximal exposure of the rectum, anus, and perineal region
- Uses abdominal flexion to enhance surgical access
- Preferred for complex anorectal and colorectal procedures
2. Lateral position
- Patient lies on their side (right or left lateral)
- Common in endoscopic and diagnostic procedures
- Provides moderate access but limited deep pelvic exposure
For example, in flexible sigmoidoscopy, the lateral position is often sufficient, but it is inadequate for deep anorectal surgical procedures requiring full exposure.
3. Supine position
- Patient lies flat on the back
- Widely used in abdominal surgery
- Limited access to posterior pelvic structures
In contrast, the Jackknife Position provides superior posterior access compared to the supine setup, especially in rectal surgery.
4. Other alternative positions
- Lithotomy position: commonly used in gynecologic and some colorectal procedures
- Sitting position: used primarily in neurosurgical or select spine procedures
Key comparative summary
- Jackknife Position → best for deep anorectal exposure
- Lateral position → diagnostic or limited access
- Supine position → general abdominal access
Anesthesia and Spinal Considerations in Jackknife Positioning
The Jackknife Position introduces a unique set of anesthetic challenges because it combines significant patient positioning adjustments with procedures that often involve the lower gastrointestinal tract. In anorectal and colorectal surgeries, anesthetic planning must account not only for the pharmacological effects of agents used but also for how the position during surgery influences physiological stability. The interaction between surgical positioning, ventilation, and circulation makes anesthesia management a critical component of safe operative care, particularly in the prone jackknife position.
Spinal anesthesia and spinal anaesthesia in prone jackknife positioning
Spinal anesthesia and spinal anaesthesia are commonly used regional techniques in lower abdominal and perineal procedures, including anorectal procedures. However, their application in the Jackknife Position requires careful sequencing and physiological awareness.
1. Timing and administration
In most clinical settings:
- Spinal anesthesia is administered before the patient is placed in the prone orientation
- The block is typically performed in a supine position or occasionally in a lateral position
- Once adequate sensory level is achieved, the patient is placed into the prone jackknife position
2. Clinical rationale
The rationale for this approach includes:
- Avoiding difficulty in spinal needle placement after positioning
- Ensuring stable anesthetic spread before surgical manipulation
- Reducing risk of patient movement during positioning
3. Effects on anesthetic spread
The Jackknife Position may influence:
- Distribution of local anesthetic in the cerebrospinal fluid
- Sympathetic blockade levels
- Duration and intensity of the spinal block
For example, a patient undergoing hemorrhoidectomy under spinal anesthesia may experience more pronounced hypotension after being moved into the jackknife configuration due to altered venous return.
Anesthetic implications during anorectal surgery in jackknife position
The Jackknife Position significantly affects both respiratory and cardiovascular physiology during anorectal surgeries, making anesthetic management more complex.
1. Hemodynamic effects
The flexed positioning of the abdomen can lead to:
- Reduced venous return to the heart
- Decreased cardiac output in prolonged procedures
- Fluctuations in blood pressure requiring intraoperative adjustment
These hemodynamic changes jackknife prone position are especially relevant in patients with cardiovascular comorbidities.
2. Respiratory considerations
Respiratory mechanics are also affected due to:
- Compression of the abdomen against the diaphragm
- Reduced lung expansion capacity
- Increased airway pressures during ventilation
This is particularly important when general anesthesia or general endotracheal anesthesia is used.
3. Choice of anesthetic technique
Depending on procedure complexity, anesthesia may include:
- Regional techniques (spinal anesthesia)
- Sedation with monitored anesthesia care
- Full general anesthesia for complex colorectal interventions
For example, during abdominoperineal resection, general anesthesia is often preferred due to prolonged duration and extensive dissection requirements.
4. Monitoring requirements
Continuous intraoperative monitoring is essential:
- Blood pressure and mean arterial pressure
- Oxygen saturation
- End-tidal CO₂ levels
- Cardiac rhythm
These parameters help detect early instability related to positioning and anesthesia interaction.
Patient position considerations for anesthetic stability in colorectal and anal procedures
Maintaining anesthetic stability in the Jackknife Position requires precise coordination between the anesthesia provider and the surgical team, particularly in colorectal surgeries and anal procedures.
1. Positioning safety before and after anesthesia
Key steps include:
- Ensuring the airway is secured before full prone positioning
- Confirming correct spinal alignment after repositioning
- Verifying that no excessive abdominal compression is present
This ensures the patient position supports both surgical access and physiological stability.
2. Impact of positioning on anesthetic stability
The position provides both advantages and risks:
Advantages:
- Improved surgical exposure reduces operative time
- Better access allows more efficient procedural flow
Risks:
- Potential respiratory restriction due to abdominal flexion
- Altered venous return affecting blood pressure
- Increased risk of pressure-related complications if not padded correctly
3. Special considerations in colorectal and anal surgery
In more complex colorectal or anal procedures:
- Longer operative duration increases anesthetic exposure
- Greater risk of fluid shifts and blood loss
- Need for careful intraoperative fluid management
For instance, during rectal tumor excision, even small changes in positioning can significantly influence ventilation and hemodynamic stability.
4. Role of the surgical and anesthesia team
Successful management depends on coordinated care:
- The surgical team ensures proper table flexion and exposure
- The anesthesia provider monitors systemic stability
- Nursing and perioperative staff ensure padding and alignment
This multidisciplinary approach ensures that the Jackknife Position remains both effective and safe throughout the procedure.
Surgical Technique and Safe Patient Positioning in Jackknife Surgery
Safe and effective use of the Jackknife Position depends on precise surgical positioning, coordinated teamwork, and careful attention to patient safety principles throughout the perioperative period. In anorectal surgeries and selected colorectal surgeries, correct positioning directly influences surgical exposure, procedural efficiency, and the risk of complications such as compression injuries or respiratory compromise. Because the prone jackknife position involves significant flexion of the body, it requires a structured and systematic approach from the surgical and anesthesia teams to ensure that the patient position supports both operative access and physiological stability.
Step-by-step patient positioning in the prone jackknife position during surgery
Establishing the Jackknife Position follows a controlled sequence that ensures both safety and optimal surgical exposure of the rectum, anus, and surrounding structures.
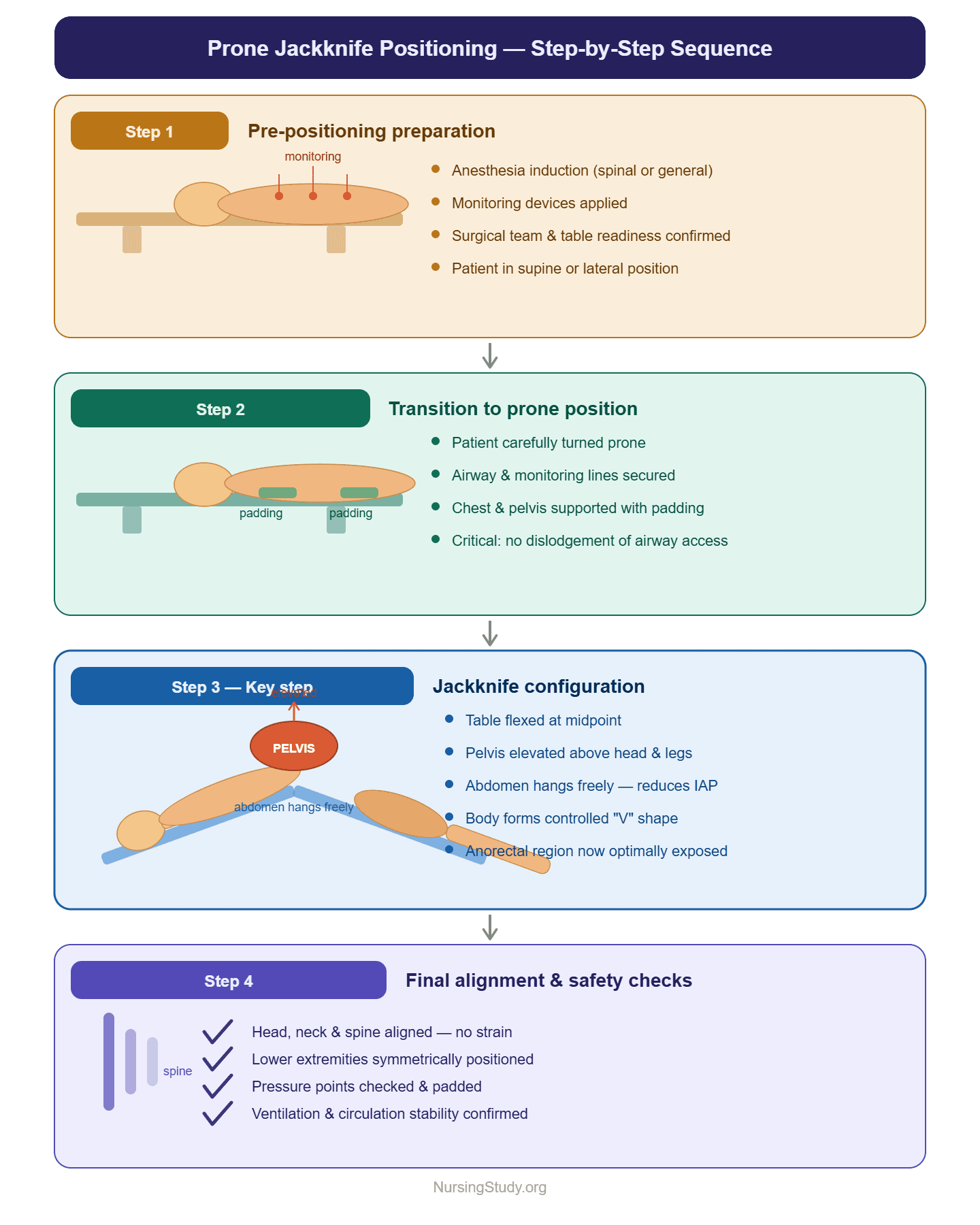
1. Pre-positioning preparation
Before any movement:
- The patient undergoes induction of anesthesia (spinal or general depending on the case)
- Monitoring devices are applied for continuous assessment of vital signs
- The surgical team confirms readiness of the operating room and operating table
At this stage, the patient is placed in a standard supine or lateral orientation depending on anesthetic technique.
2. Transition to prone position
- The patient is carefully turned into a prone position
- Airway and monitoring lines are secured and checked
- The chest and pelvis are supported using appropriate padding
This step is critical to prevent accidental dislodgement of airway or vascular access.
3. Formation of the jackknife configuration
- The operating table is flexed at the midpoint
- The pelvis is elevated above the level of the head and legs
- The abdomen is allowed to hang freely to reduce intra-abdominal pressure
- The body assumes a controlled “V” shape characteristic of the prone jackknife position
This configuration enhances exposure for anorectal procedures by improving access to the surgical site.
4. Final alignment and safety checks
- Head, neck, and spine are aligned to prevent strain
- Lower extremities are positioned symmetrically
- Pressure points are checked and padded
- Final confirmation of ventilation and circulation stability is performed
This ensures the position during surgery is both anatomically effective and physiologically safe.
Surgical aids and operating table adjustments for anorectal exposure
The effectiveness of the Jackknife Position is significantly enhanced by specialized equipment and careful adjustment of the surgical table.
1. Operating table adjustments
Modern operating tables allow:
- Controlled flexion to achieve optimal jackknife angle
- Adjustable height and tilt for surgeon ergonomics
- Stability locking mechanisms to maintain position throughout the procedure
These adjustments are essential in anorectal surgical procedures, where precision exposure of the rectal and anal region is required.
2. Positioning aids and support devices
Common aids include:
- Gel pads to reduce pressure on bony prominences
- Chest rolls to support respiratory mechanics
- Pelvic bolsters to maintain elevation
- Arm boards to prevent shoulder strain
These devices ensure that the position provides both surgical access and physical protection.
3. Enhancing surgical exposure
The combination of table flexion and positioning aids:
- Improves visualization of the anus and perineal region
- Facilitates access during resection procedures
- Reduces need for excessive tissue retraction
- Enhances precision in delicate colorectal surgeries
For example, during hemorrhoidectomy, optimal table flexion allows the surgeon to clearly visualize internal and external hemorrhoidal tissue with minimal obstruction.
Prevention of pressure injuries and nerve compression in jackknife prone position
Because the Jackknife Position involves prolonged flexion and pressure redistribution, preventing injury is a critical component of perioperative care.
1. Risk factors for injury
The position may increase risk of:
- Peripheral nerve compression
- Pressure ulcers over bony prominences
- Musculoskeletal strain
- Vascular compromise in dependent areas
These risks are heightened in long operative procedures or in patients with reduced mobility.
2. Prevention strategies
To reduce complications, the following measures are implemented:
a. Padding and support
- Adequate padding is placed under knees, hips, chest, and elbows
- Soft supports are used to distribute weight evenly
- Special attention is given to the lower extremities
b. Avoidance of excessive flexion
- Over-flexion of the abdomen is avoided
- The flex angle is adjusted to balance exposure and safety
- Continuous reassessment ensures alignment remains appropriate
c. Nerve protection
- Careful positioning of arms prevents brachial plexus injury
- Lower limb positioning avoids peroneal nerve compression
- Regular intraoperative checks are performed by the surgical team
3. Monitoring during surgery
Throughout the procedure:
- Skin integrity is assessed when possible
- Perfusion status is monitored indirectly through vital signs
- Anesthesia providers watch for signs of compromised circulation
4. Postoperative considerations
After surgery:
- Early assessment for neuropathy or pressure injury is essential
- Documentation of positioning-related risk factors is completed
- Recovery care includes monitoring for delayed complications
For example, a patient undergoing prolonged colorectal resection in the prone jackknife position may require extended postoperative evaluation for lower limb sensory changes due to positioning-related nerve stress.
Hemodynamics, Risks, and Intraoperative Considerations
The Jackknife Position introduces important physiological challenges during anorectal surgeries and colorectal surgeries because it alters both cardiovascular and respiratory dynamics. In perioperative practice, maintaining stability during the position during surgery is essential, as even small changes in posture can significantly influence hemodynamics, ventilation, and tissue perfusion. The prone jackknife position is particularly impactful because it combines prone orientation with marked flexion at the abdomen and hips, creating both mechanical advantages for surgical exposure and physiological stress on the patient.
Hemodynamic changes associated with prone jackknife positioning
The Jackknife Position produces distinct hemodynamic changes jackknife prone position due to gravitational shifts, abdominal compression, and altered venous return. These changes are clinically significant, especially in prolonged operative procedures.
1. Reduction in venous return
- Abdominal flexion increases intra-abdominal pressure
- Compression of the inferior vena cava may occur
- Venous return to the heart is reduced
This can lead to:
- Decreased preload
- Lower cardiac output
- Transient hypotension during positioning or intraoperative manipulation
2. Changes in blood pressure regulation
- Blood pressure may fluctuate during transition into the prone jackknife position
- Reflex compensatory mechanisms may be blunted under general anesthesia
- Patients with cardiovascular disease are particularly sensitive
3. Impact on mean arterial pressure
- Mean arterial pressure may decrease due to reduced cardiac output
- Continuous monitoring is required to ensure adequate organ perfusion
- Fluid management may be adjusted intraoperatively
4. Clinical example
During a prolonged abdominoperineal resection, a patient in the Jackknife Position may experience gradual hypotension as abdominal compression reduces venous return, requiring vasopressor support or fluid optimization by the anesthesia team.
Respiratory effects and physiologic impact of jackknife position
The Jackknife Position also significantly affects respiratory mechanics due to its flexed configuration and abdominal positioning.
1. Restriction of diaphragmatic movement
- Abdominal contents are displaced upward against the diaphragm
- Diaphragmatic excursion is reduced
- Lung expansion becomes mechanically limited
2. Decreased lung compliance
- Chest wall mechanics are altered in the prone flexed position
- Compliance decreases, particularly in obese or elderly patients
- Increased airway pressures may be required during ventilation
3. Ventilation-perfusion imbalance
- Redistribution of pulmonary blood flow may occur
- Basal lung regions may receive reduced ventilation
- Risk of mild hypoxemia in prolonged procedures increases
4. Airway management considerations
In cases requiring general endotracheal anesthesia:
- Secure airway placement is essential before positioning
- Endotracheal tube displacement must be carefully monitored
- Ventilator adjustments may be needed to maintain oxygenation
5. Clinical example
In a patient undergoing complex colorectal surgery, the anesthetic team may observe increased peak airway pressures after transitioning into the jackknife configuration due to abdominal compression limiting diaphragmatic movement.
Intraoperative risks in anorectal and colorectal surgical procedures
While the Jackknife Position provides excellent exposure for anorectal procedures, it also introduces several intraoperative risks that must be actively managed by the surgical and anesthesia teams.
1. Cardiovascular instability
- Hypotension due to reduced venous return
- Bradycardia in response to autonomic changes
- Fluctuating hemodynamic responses during surgical manipulation
These risks require:
- Continuous cardiovascular monitoring
- Prompt fluid or pharmacologic intervention when needed
2. Respiratory compromise
- Reduced tidal volume during ventilation
- Increased airway pressure requirements
- Risk of hypoventilation if adjustments are not made
3. Nerve compression and musculoskeletal injury
- Prolonged pressure on peripheral nerves
- Potential brachial plexus or peroneal nerve injury
- Risk increases with long operating time
4. Pressure-related injuries
- Skin breakdown over bony prominences
- Tissue ischemia due to sustained compression
- Higher risk in prolonged colorectal or rectal procedures
5. Surgical access-related risks
- Over-flexion may distort anatomical landmarks
- Excessive tension may affect the surgical site visibility
- Improper positioning can reduce efficiency of resection procedures
6. Clinical example
During a long colorectal resection for rectal cancer, prolonged time in the prone jackknife position may lead to gradual hypotension, requiring adjustments in anesthesia depth and fluid therapy, while the surgical team intermittently reassesses positioning to avoid excessive abdominal compression.
Patient Selection, Preparation, and Perioperative Care
The safe and effective use of the Jackknife Position in anorectal surgeries and colorectal surgeries depends not only on technical positioning skills but also on appropriate patient selection, thorough preoperative preparation, and structured perioperative care. Because the prone jackknife position significantly alters hemodynamics, respiratory mechanics, and tissue pressure distribution, careful evaluation of the patient position suitability is essential to reduce intraoperative and postoperative complications. In clinical practice, outcomes are strongly influenced by how well patients are assessed and prepared before being placed into this specialized position during surgery.
Patient selection criteria for jackknife prone position surgery
Not all patients are suitable candidates for surgery performed in the Jackknife Position, particularly when prolonged operative time or complex anorectal procedures are anticipated. Patient selection is therefore based on a combination of physiological stability, surgical indication, and anesthetic risk.
1. Cardiopulmonary stability
Patients must have adequate cardiovascular and respiratory reserve because the prone jackknife position can:
- Reduce venous return due to abdominal compression
- Affect cardiac output and hemodynamics
- Restrict lung expansion and ventilation efficiency
Patients with severe heart failure, uncontrolled hypertension, or advanced chronic obstructive pulmonary disease may require alternative positioning such as lateral position or supine position depending on the surgical procedure.
2. ASA physical status classification
The American Society of Anesthesiologists classification system is commonly used:
- ASA I–II: Generally suitable for Jackknife Position
- ASA III: Requires careful risk-benefit evaluation
- ASA IV and above: High risk; alternative positioning may be preferred
3. Surgical indication
The Jackknife Position is most appropriate for:
- Hemorrhoidectomy
- Fistula-in-ano repair
- Perianal abscess drainage
- Complex rectal and anorectal diseases requiring deep exposure
4. Body habitus and mobility
- Obesity increases risk of respiratory compromise in prone flexion
- Limited spinal mobility may complicate safe transition into position
- Patients with musculoskeletal disorders may require modified positioning strategies
Preoperative preparation and positioning planning in anorectal surgeries
Effective preoperative preparation is essential to ensure safe transition into the prone jackknife position and to optimize surgical outcomes in anorectal surgeries.
1. Preoperative assessment and planning
Preparation begins with a structured evaluation:
- Review of medical history and comorbidities
- Assessment of airway and anesthetic risk
- Identification of potential positioning limitations
- Planning of spinal anesthesia or general anesthesia approach
2. Coordination between surgical and anesthesia teams
Successful positioning requires multidisciplinary coordination:
- The surgical team determines exposure requirements for the surgical site
- The anesthesia team anticipates changes in respiratory and cardiovascular function
- Nursing staff prepare the operating room and operating table for adjustment
3. Positioning strategy development
Before induction, the team plans:
- Degree of table flexion required for optimal exposure
- Padding placement to prevent compression injuries
- Alignment of head and legs to maintain spinal neutrality
- Airway protection strategy if general endotracheal anesthesia is used
4. Patient education and consent
Although not always emphasized, patient understanding is important:
- Explanation of the position during surgery
- Discussion of postoperative expectations
- Clarification of potential risks such as discomfort or temporary soreness
5. Example
In a patient scheduled for hemorrhoidectomy, preoperative planning may involve selecting spinal anesthesia, preparing a flexed operating table setup, and ensuring gel padding is available to support the pelvis and prevent pressure injury once the patient is placed in the Jackknife Position.
Perioperative and postoperative care following jackknife positioning
Care does not end once the surgical procedure is completed; both perioperative and postoperative phases are critical for ensuring safety and recovery after use of the Jackknife Position.
1. Intraoperative (perioperative) care considerations
During surgery, continuous monitoring is essential to maintain stability:
- Hemodynamic monitoring
- Blood pressure fluctuations due to positional changes
- Monitoring of mean arterial pressure
- Early detection of hypovolemia or instability
- Respiratory monitoring
- Ventilation adjustments in response to abdominal compression
- Oxygen saturation tracking
- Airway security in cases using general anesthesia
- Positioning surveillance
- Ensuring no excessive flex or abdominal strain
- Checking for limb alignment and pressure points
- Preventing prolonged compression of nerves or vessels
2. Immediate postoperative care
After completion of the surgical procedure, attention shifts to safe recovery from both anesthesia and positioning effects:
- Gradual repositioning from prone to supine or recovery position
- Monitoring for residual effects of spinal anesthesia or general anesthesia
- Assessment of pain, especially in pressure areas
3. Monitoring for positioning-related complications
Patients who undergo prolonged prone jackknife position surgery must be assessed for:
- Peripheral nerve dysfunction (numbness or weakness)
- Pressure-related skin injury
- Musculoskeletal discomfort
- Delayed respiratory recovery
4. Postoperative recovery in anorectal surgeries
In anorectal procedures, recovery care includes:
- Pain control strategies tailored to perianal sensitivity
- Wound care and hygiene management
- Monitoring for bleeding or infection at the surgical site
- Early mobilization to reduce complications
5. Clinical example
A patient recovering from a colorectal surgery performed in the Jackknife Position may initially experience lower back discomfort and mild leg paresthesia due to prolonged positioning. With appropriate postoperative assessment, these symptoms are typically transient and resolve with supportive care and repositioning.
Evidence-Based Practice and Research in Jackknife Positioning
The Jackknife Position has evolved from a primarily technical surgical setup into a well-studied component of evidence-based perioperative care, particularly in anorectal surgeries and selected colorectal surgeries. In modern surgical practice, decisions regarding surgical positioning are increasingly guided by clinical research, comparative outcome data, and anesthetic safety profiles rather than tradition alone. This shift toward evidence-based practice has helped refine how the prone jackknife position is applied in surgical procedure planning, especially in procedures involving the rectum, anus, and surrounding perineal structures.
Clinical outcomes of jackknife position in anorectal surgery
Clinical outcomes associated with the Jackknife Position are generally evaluated in terms of surgical exposure, procedural efficiency, complication rates, and recovery quality following anorectal procedures.
1. Improved surgical exposure and precision
One of the most consistently reported benefits is enhanced visualization of the operative field:
- Direct access to the anal canal and rectal vault
- Reduced obstruction from abdominal contents
- Improved accuracy during delicate dissection and resection procedures
For example, in hemorrhoidectomy procedures, the prone jackknife position allows the surgeon to clearly identify vascular pedicles, improving precision and reducing operative difficulty.
2. Reduced operative difficulty and time
Studies in anorectal surgeries frequently report:
- Shorter operating time due to improved exposure
- Reduced need for excessive retraction
- More efficient instrument handling
This is particularly important in ambulatory surgery, where procedural efficiency directly affects turnover and recovery flow.
3. Postoperative outcomes
Clinical outcomes also extend into the postoperative period:
- Reduced wound tension in perineal regions
- Comparable or improved pain control compared to alternative positions
- Low incidence of position-related complications when properly executed
However, improper positioning may still lead to postoperative complications such as nerve irritation or pressure-related discomfort.
4. Example application
In a patient undergoing fistula-in-ano repair, the Jackknife Position improves fistula tract visualization, allowing complete excision while minimizing tissue trauma and reducing recurrence risk.
Comparative studies and randomized controlled trial evidence on surgical positioning
Evidence-based evaluation of the Jackknife Position often involves comparison with alternative patient positions such as the lithotomy position, lateral position, and supine position. These comparative studies and randomized controlled trial designs provide valuable insights into clinical decision-making.
1. Jackknife position versus lithotomy position
Research comparing the prone jackknife position with the lithotomy position in anorectal surgeries shows:
- Better posterior pelvic exposure in Jackknife Position
- Reduced need for excessive limb manipulation
- Lower risk of lower limb neurovascular strain compared to prolonged lithotomy positioning
However, lithotomy may still be preferred for combined abdominal-perineal procedures requiring dual access.
2. Jackknife position versus lateral position
Comparisons with the lateral position reveal:
- Jackknife provides superior access to deep anorectal structures
- Lateral positioning is more comfortable for shorter diagnostic procedures
- Jackknife is more effective for complex colorectal surgeries requiring full exposure
3. Randomized controlled trial findings
Randomized controlled trial evidence in surgical positioning highlights:
- Improved surgical field visibility in Jackknife Position
- Similar or slightly increased anesthetic complexity due to hemodynamics changes
- No significant increase in major complications when properly executed
These findings support its continued use in appropriately selected patients.
4. Hemodynamic and anesthetic comparison outcomes
Across studies:
- Slight reductions in mean arterial pressure may occur in Jackknife Position
- Increased ventilatory pressures may be required compared to supine positioning
- These effects are generally manageable with intraoperative monitoring
For example, during abdominoperineal resection, studies show that while the Jackknife Position may require more careful anesthetic titration, it significantly improves surgical access and reduces operative difficulty.
Future directions in surgical positioning and anesthesia practice
The future of surgical positioning, including the Jackknife Position, is increasingly shaped by advances in technology, perioperative monitoring, and minimally invasive techniques.
1. Improved ergonomic operating tables
Modern innovations in operating table design are focusing on:
- Automated and precise flexion control for prone jackknife position
- Integrated pressure distribution systems to reduce compression injuries
- Enhanced stability during prolonged operative procedures
These improvements aim to enhance both patient safety and surgical efficiency.
2. Enhanced anesthetic monitoring and management
Advancements in anesthesia care include:
- Real-time hemodynamic monitoring systems
- Improved ventilation algorithms for prone positioning
- Better prediction of hemodynamic changes jackknife prone position
These tools help mitigate risks associated with prolonged positioning.
3. Minimally invasive and ambulatory surgical trends
With the rise of ambulatory anorectal surgery:
- There is increasing emphasis on shorter operative durations
- Less invasive anorectal procedures are reducing positioning duration
- Enhanced recovery protocols are being integrated with positioning strategies
For example, minimally invasive hemorrhoid procedures may still use the Jackknife Position but for shorter durations with reduced physiological strain.
4. Integration of evidence-based guidelines
Future clinical practice is moving toward:
- Standardized protocols for surgical positioning
- Evidence-based selection of patient position based on comorbidities
- Greater reliance on comparative outcome data from randomized controlled trial research
5. Example of future application
In a modern colorectal unit, a patient undergoing rectal cancer surgery may benefit from a hybrid approach where the Jackknife Position is combined with enhanced monitoring systems and dynamic table adjustments to reduce physiological stress while maintaining optimal surgical exposure.
Behind on multiple nursing assignments?
Our team will handle them while you focus on learning and clinical work.
Conclusion
The Jackknife Position remains a highly specialized and clinically significant form of surgical positioning in modern operative care, particularly within anorectal surgeries and selected colorectal surgeries. Its structured modification of the prone position allows superior exposure of the rectum, anus, and surrounding perineal structures, making it indispensable for a wide range of surgical procedures, including hemorrhoidectomy, fistula repair, and complex rectal resections. When properly applied, the prone jackknife position enhances surgical precision, improves visualization of the operative field, and supports efficient access during technically demanding interventions.
Across all phases of care, the effectiveness of the Jackknife Position is determined not only by technical setup but also by integrated perioperative management. Careful attention to patient position, anesthetic planning, and intraoperative monitoring is essential due to the position’s influence on hemodynamics, respiratory mechanics, and tissue perfusion. The interaction between positioning and spinal anesthesia, as well as general anesthetic techniques, highlights the importance of coordinated multidisciplinary care in maintaining physiological stability throughout surgery.
At the same time, the clinical advantages of the Jackknife Position must be balanced against its inherent risks, including compression, respiratory restriction, and position-related complications. These challenges underscore the importance of meticulous surgical positioning, structured patient selection, and vigilant perioperative care. When these safeguards are implemented, the position demonstrates a strong safety profile with favorable outcomes in both ambulatory anorectal surgery and complex inpatient procedures.
Evidence-based practice continues to reinforce the role of the Jackknife Position, with comparative studies and randomized controlled trial data supporting its superiority in specific surgical contexts, particularly where deep pelvic exposure is required. As surgical technology advances, improvements in operating table design, anesthetic monitoring, and perioperative protocols are expected to further enhance both the safety and effectiveness of this positioning technique.
Ultimately, the Jackknife Position represents a convergence of surgical precision, anesthetic science, and perioperative nursing care. Its continued use in modern practice reflects not only its technical utility but also the evolving understanding of how positioning directly influences surgical outcomes, patient safety, and overall procedural success in anorectal and colorectal surgery.
Frequently Asked Questions
What are the 4 types of position?
In nursing and clinical practice, patient positioning is commonly grouped into four broad categories:
- Supine position – patient lies flat on the back
- Prone position – patient lies face down
- Lateral position – patient lies on the side (right or left)
- Fowler’s position – patient is semi-sitting with head of bed elevated
These foundational positions are modified in practice to meet specific surgical or medical needs.
What are the 10 positions used in nursing?
Commonly taught nursing and clinical positioning includes:
- Supine position
- Prone position
- Lateral position (right/left lateral)
- Fowler’s position
- High Fowler’s position
- Semi-Fowler’s position
- Lithotomy position
- Sims’ position
- Trendelenburg position
- Reverse Trendelenburg position
These positions are used to improve comfort, breathing, circulation, and access for procedures.
What is an example of a prone position?
An example of a prone position is:
- A patient lying face down on an operating table during spinal surgery or back procedures
Another clinical example is:
- A patient placed prone in intensive care to improve oxygenation in severe respiratory distress (prone ventilation)
Why is it called jackknife position?
It is called the Jackknife Position because the body is flexed in a way that resembles a folding pocket knife being closed:
- The patient lies prone
- The hips are elevated
- The body is sharply flexed at the abdomen
This creates a “V-shaped” or “hinged” posture, similar to how a jackknife folds, which improves exposure of the rectum and anal region during surgery.