
Orthopneic Position 101: Position, Orthopneic Position, Tripod Position, Orthopnea, and Clinical Application in Nursing Care
The orthopneic position is an important clinical positioning technique used in respiratory care to support patients experiencing difficulty breathing, particularly when symptoms worsen in the supine or recumbent position. It is commonly observed in individuals with orthopnea, shortness of breath, and varying degrees of respiratory distress, where the body naturally adapts by assuming a forward-leaning sitting posture to improve ventilation and reduce the effort required for breathing. In clinical settings, this position is not only a comfort measure but also a significant indicator of underlying cardiopulmonary compromise.
The role of the orthopneic position in respiratory function can be understood through its impact on the lungs, diaphragm, and overall breathing mechanics. By shifting the body into a supported sitting position, often with the upper body leaning forward and supported by a pillow, bedside table, or the knees, the position enhances lung expansion and improves airflow. This adjustment reduces pressure on the diaphragm, allowing it to move more effectively during inhalation and exhalation. As a result, patients often report reduced breathlessness and an improved ability to breathe more comfortably.
Key clinical characteristics of this position include the following:
- Postural alignment
- The patient assumes a sitting position, typically at the edge of the bed or in a chair.
- The trunk is inclined forward to reduce thoracic restriction.
- The head of the bed may be elevated to support breathing effort.
- Upper limb support
- Arms are positioned on a stable surface such as:
- A pillow placed on a bedside table
- The knees in a tripod-like stance
- This support helps stabilize the shoulder girdle and accessory respiratory muscles.
- Arms are positioned on a stable surface such as:
- Respiratory adaptation
- Accessory muscles of respiration are actively engaged.
- There is reduced diaphragmatic load, improving chest wall expansion.
- Patients often exhibit visibly reduced work of breathing.
From a clinical perspective, this positioning is closely associated with conditions such as chronic obstructive pulmonary disease, pulmonary edema, heart failure, and acute respiratory conditions where fluid overload or airway obstruction contributes to impaired gas exchange. In such cases, patients often present with orthopnea, a type of dyspnea characterized by shortness of breath that worsens when lying flat and improves when sitting upright.
Overall, the orthopneic position represents an essential adaptive mechanism in respiratory care, demonstrating how body positioning can directly influence cardiopulmonary efficiency. Understanding its characteristics and physiological basis is crucial for recognizing respiratory compromise early and supporting patients through appropriate non-pharmacological interventions that promote more effective breathing patterns.
Not confident in your nursing writing skills?
We’ll produce clear, professional, and evidence-based work.
Understanding the Orthopneic Position and Its Role in Relieving Orthopnea and Shortness of Breath
The Orthopneic Position is a therapeutic and compensatory body posture that plays a critical role in relieving orthopnea, a type of dyspnea (shortness of breath) that worsens when a patient lies flat and is relieved by sitting upright. In clinical practice, the Orthopneic Position is most commonly observed in patients who are experiencing breathing difficulties, particularly during episodes of acute respiratory distress, where lying in a recumbent position significantly worsens ventilation and gas exchange.
At its core, the Orthopneic Position functions as a physiological adaptation that helps improve the interaction between the lungs, diaphragm, and accessory muscles of respiration. When a patient assumes the Orthopneic Position, usually by sitting upright and leaning forward, there is a noticeable reduction in the workload of the respiratory system, allowing the patient to breathe more efficiently and experience relief from shortness of breath.
How the Orthopneic Position Relieves Orthopnea and Shortness of Breath
The effectiveness of the Orthopneic Position in relieving symptoms is based on several interconnected physiological mechanisms:
- Improved Lung Expansion
- When sitting upright, the lung capacity increases due to reduced compression from abdominal organs.
- This allows for greater tidal volume and improved oxygen exchange.
- Patients with conditions such as COPD (chronic obstructive pulmonary disease) often report that the Orthopneic Position significantly improves their ability to “breathe better.”
- Reduced Diaphragmatic Pressure
- In a supine position, abdominal contents push upward against the diaphragm, limiting its movement.
- The Orthopneic Position allows the diaphragm to descend more freely during inspiration.
- This is especially beneficial in patients with heart failure or chronic kidney disease, where fluid overload increases abdominal and thoracic pressure.
- Optimization of Heart and Lung Function
- In conditions like pulmonary edema, fluid accumulation in the lungs impairs oxygen exchange.
- Sitting upright reduces venous return and pulmonary congestion, easing the strain on the heart and lungs.
- This helps relieve the sensation of breathlessness commonly seen in these patients.
- Engagement of Accessory Muscles
- The Orthopneic Position allows the use of accessory respiratory muscles in the neck and shoulders.
- This compensates for weakened or overloaded primary respiratory muscles.
- Patients often instinctively place their arms on a support surface to stabilize these muscles.
- Reduction of Work of Breathing
- By improving chest wall mechanics, the Orthopneic Position reduces the energy required for each breath.
- This is particularly important during episodes of acute respiratory distress syndrome (ARDS) or severe infection-related respiratory compromise.
Clinical Example
A patient with congestive heart failure may report that they experience shortness of breath when lying flat, a classic symptom of orthopnea. When placed in the Orthopneic Position—sitting upright at the edge of the bed, leaning forward with arms supported on a pillow or overbed table—the patient often reports immediate relief. Oxygen saturation may also improve due to enhanced ventilation-perfusion matching.
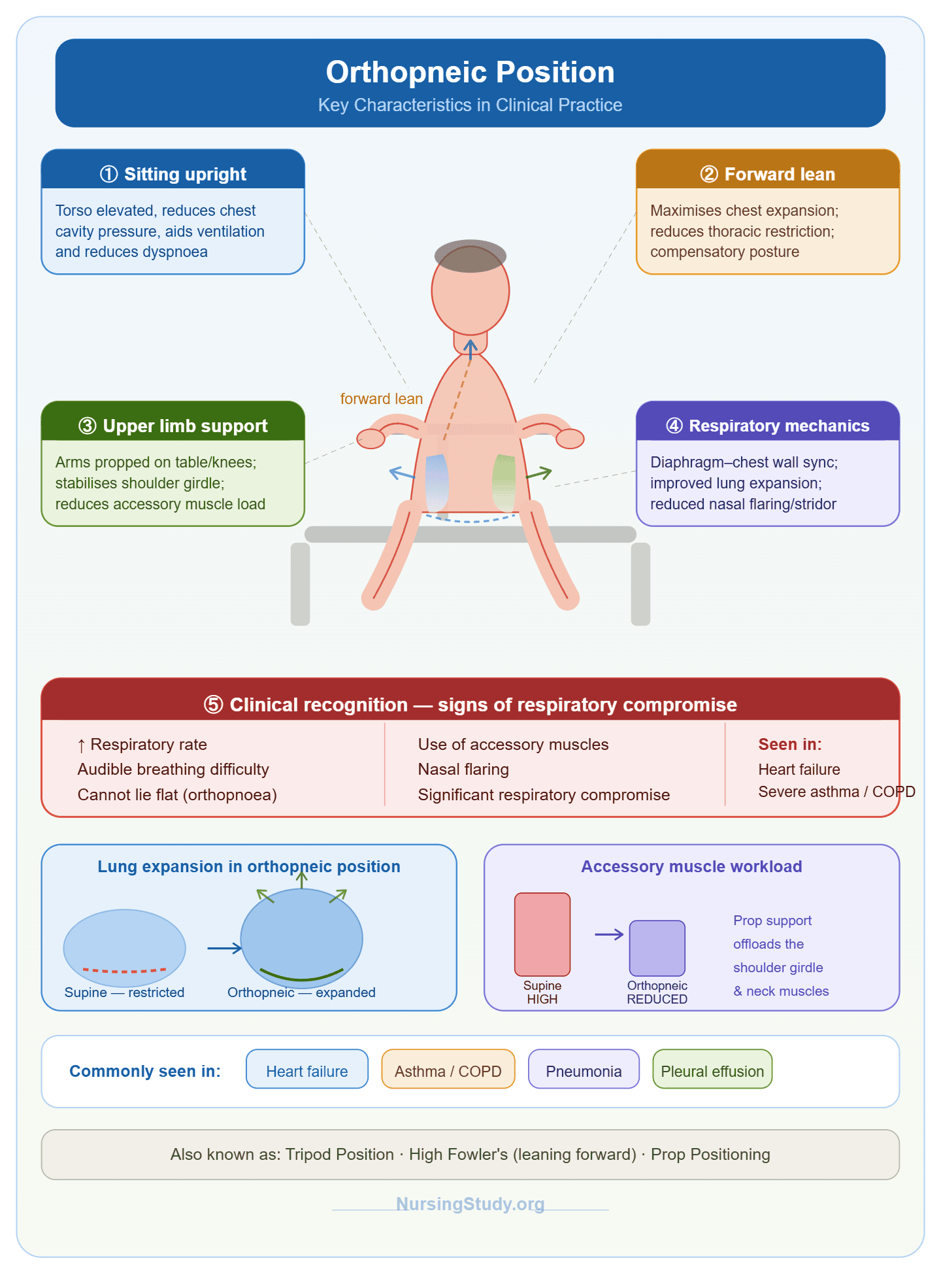
Key Characteristics of the Orthopneic Position in Clinical Practice
The Orthopneic Position is defined not only by its therapeutic effect but also by its consistent postural characteristics observed in clinical settings. These features are important for identifying patients who are instinctively using this position to manage difficulty breathing.
1. Sitting Upright Posture
- The patient assumes a sitting position, often at the side of the bed or in a chair.
- The torso is elevated, sometimes supported by the head of the bed or multiple pillows.
- This upright alignment reduces pressure on the chest cavity and improves ventilation.
2. Forward Leaning Alignment
- The patient naturally leans forward to maximize chest expansion.
- This forward posture reduces restriction on the thoracic cavity.
- It is commonly referred to as a compensatory posture for breathlessness.
3. Upper Limb Support (Prop Positioning)
- The arms are placed on a stable surface such as:
- An overbed table
- The knees
- A bedside pillow or armrest
- This “prop” support stabilizes the shoulder girdle and reduces the effort required by accessory muscles.
4. Enhanced Respiratory Mechanics
- The position promotes better synchronization of the diaphragm and chest wall.
- It improves lung expansion, especially in patients with restricted airflow.
- It helps reduce visible signs of respiratory distress, such as nasal flaring or use of accessory muscles.
5. Clinical Recognition of Respiratory Distress
- Patients using the Orthopneic Position often present with:
- Increased respiratory rate
- Audible breathing difficulties
- Inability to tolerate lying flat
- This position is frequently a sign that the patient is experiencing significant respiratory compromise.
Clinical Example
A patient with chronic obstructive pulmonary disease experiencing an exacerbation may sit at the edge of the bed, leaning forward with elbows resting on a pillow placed on an overbed table. This posture is instinctively adopted because it helps reduce air trapping and improves expiratory flow, making breathing less labored.
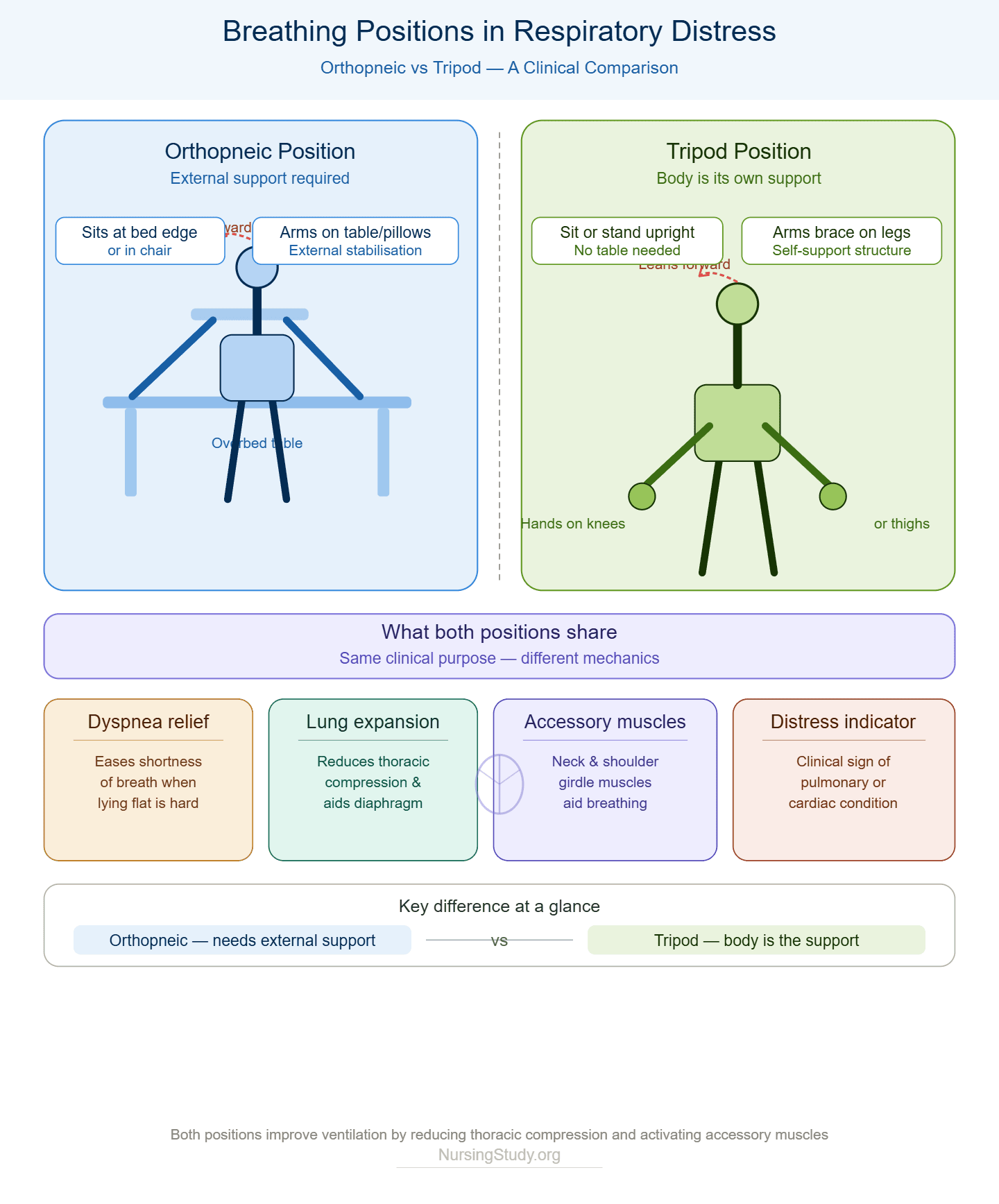
Orthopneic Position vs Tripod Position: Differences, Similarities, and Clinical Significance
The Orthopneic Position and the tripod position are closely related respiratory support postures commonly observed in patients experiencing shortness of breath, breathlessness, and other forms of respiratory distress. Although they are often used interchangeably in informal clinical discussions, they are not identical. Each represents a distinct compensatory mechanism that helps patients optimize breathing efficiency when facing different levels and causes of respiratory compromise.
Both positions are instinctive adaptations used by patients with orthopnea or acute difficulty breathing, especially when lying in a recumbent position worsens symptoms. However, subtle differences in posture, support mechanisms, and clinical context help distinguish the two.
1. Differences Between the Orthopneic Position and Tripod Position
1. Body Support and Posture
- Orthopneic Position
- Typically involves a sitting position at the edge of the bed or in a chair.
- The patient leans forward and rests on an external support such as an overbed table, multiple pillows, or bedside furniture.
- The emphasis is on external stabilization of the upper body.
- Tripod Position
- Involves a more active posture where the patient sits or stands and leans forward.
- The patient places arms on your knees or thighs for support.
- No external furniture is strictly required; the body itself provides the support structure.
2. Similarities Between the Orthopneic Position and Tripod Position
Despite their differences, both positions share key physiological and clinical purposes:
1. Relief of Dyspnea
- Both positions significantly relieve shortness of breath and breathlessness.
- They are commonly adopted by patients experiencing shortness of breath when lying flat.
2. Improved Respiratory Mechanics
- Both enhance lung expansion by reducing compression of the thoracic cavity.
- They improve diaphragmatic movement, allowing better air entry and exit.
3. Use of Accessory Muscles
- Patients in both positions engage accessory muscles of respiration, including:
- Neck muscles
- Shoulder girdle muscles
- This reduces the strain on the primary respiratory muscles.
4. Indicator of Respiratory Distress
- Both positions are clinical signs of respiratory distress.
- They often indicate underlying pulmonary or cardiac conditions affecting ventilation.
3. Clinical Significance of Both Positions
The Orthopneic Position and tripod position are not just comfort strategies—they are important clinical indicators used to assess the severity of illness.
1. Diagnostic Clues
- A patient who assumes the orthopneic position may be indicating:
- Severe orthopnea
- Fluid overload in heart failure or chronic kidney disease
- Reduced lung compliance
- A patient in a tripod position may suggest:
- Acute COPD exacerbation
- Severe airway obstruction
- Sudden onset acute respiratory distress
2. Monitoring Disease Progression
- Increased dependence on either position may signal worsening condition.
- For example:
- A patient progressing from sitting upright → tripod position → inability to speak full sentences may indicate escalating respiratory failure.
3. Nursing Assessment Value
These positions help clinicians evaluate:
- Severity of respiratory distress
- Level of oxygen deprivation
- Need for immediate intervention such as oxygen therapy or escalation of care
Clinical Situations Where Each Position Is Preferred
1. Orthopneic Position: Preferred Situations
The Orthopneic Position is most effective in conditions where lying flat significantly worsens breathing:
- Heart failure or chronic kidney disease
- Fluid overload leads to pulmonary congestion and fluid buildup in the lungs
- Sitting upright reduces venous return and improves breathing
- Pulmonary edema
- Improves oxygenation by reducing lung fluid pressure
- Severe orthopnea
- Patients are unable to tolerate lying flat due to shortness of breath
- Paroxysmal nocturnal dyspnea
- Sudden nighttime episodes of breathlessness relieved by sitting up
2. Tripod Position: Preferred Situations
The tripod position is commonly used in more acute or obstructive respiratory conditions:
- COPD (chronic obstructive pulmonary disease)
- Helps reduce air trapping and improves expiratory efficiency
- Acute respiratory distress
- Supports rapid breathing and reduces work of respiration
- Asthma exacerbations
- Helps open airways and improve airflow
- Emergency respiratory distress
- Often seen in pre-hospital or triage environments
Clinical Example Comparison
- A patient with heart failure or chronic kidney disease may sleep propped up on multiple pillows in a sitting position, unable to tolerate lying flat—this reflects the Orthopneic Position.
- A patient with severe COPD in the emergency department may be seen leaning forward with arms on knees, gasping for air—this reflects the tripod position.
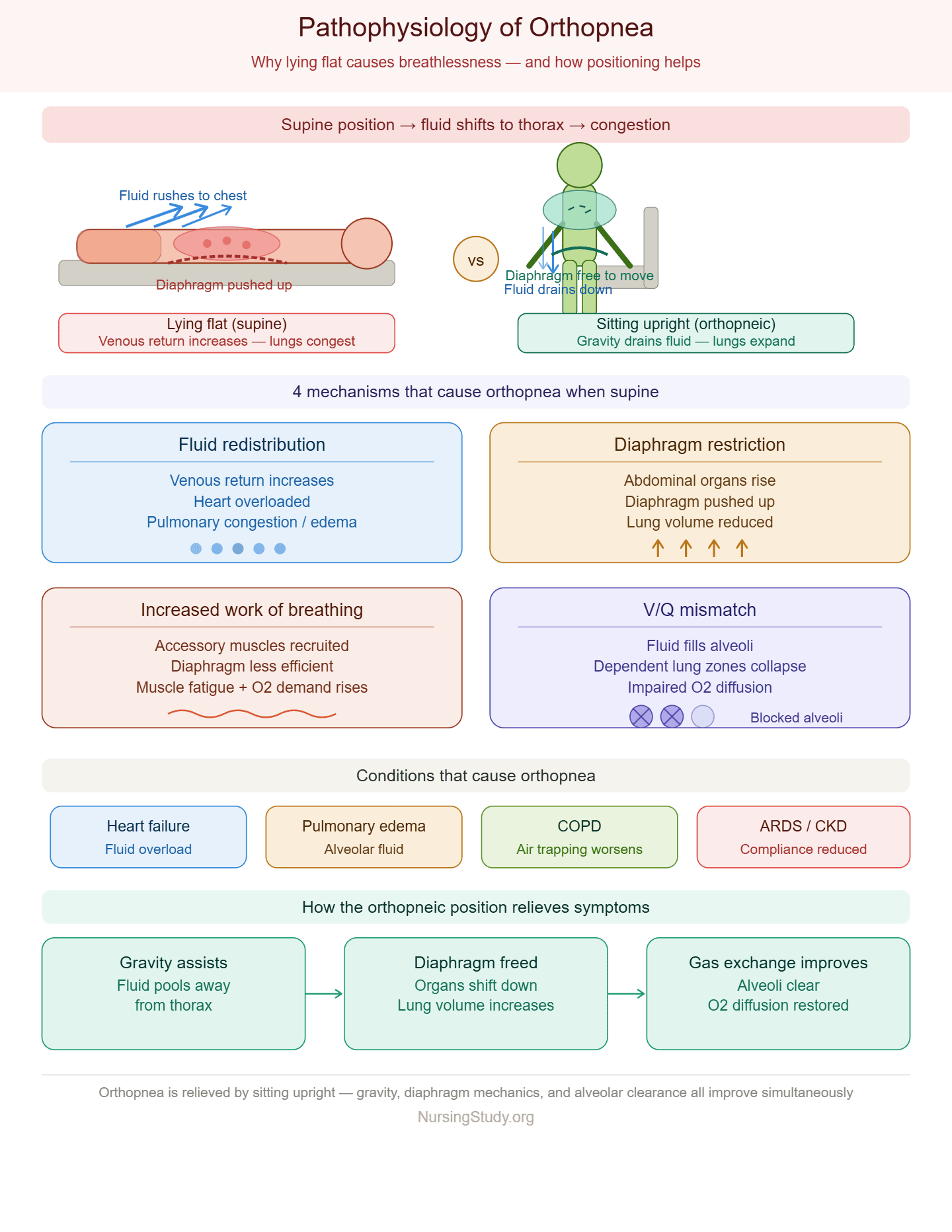
Pathophysiology of Orthopnea and Why Positioning Helps Breathing
Orthopnea is a specific type of dyspnea characterized by shortness of breath when lying flat, which is relieved by sitting upright. It is most commonly seen in patients with orthopnea related to cardiac or pulmonary conditions such as heart failure or chronic kidney disease, pulmonary edema, and advanced chronic obstructive pulmonary disease (COPD). Understanding the pathophysiology of orthopnea is essential for explaining why the Orthopneic Position is clinically effective in improving breathing.
1. Fluid Redistribution and Increased Venous Return
When a patient moves from a sitting position to a recumbent position, gravity no longer assists fluid distribution in the body. This leads to:
- Increased venous return from the legs and abdomen
- Redistribution of blood into the thoracic circulation
- Increased workload on the heart and lungs
In patients with heart failure or chronic kidney disease, the heart is unable to efficiently manage this increased volume. As a result:
- Blood backs up into the pulmonary circulation
- This causes fluid buildup in the lungs (pulmonary congestion or pulmonary edema)
- Gas exchange becomes impaired, leading to shortness of breath and breathing difficulties
This explains why orthopnea is often a condition that causes sudden breathing discomfort when lying flat.
2. Diaphragmatic Restriction and Reduced Lung Expansion
In the supine position:
- Abdominal organs shift upward toward the diaphragm
- The diaphragm is pushed upward into the thoracic cavity
- This reduces maximum chest expansion and limits lung volume
For individuals with COPD or other pulmonary conditions:
- Already compromised lung function becomes further restricted
- Air trapping worsens, increasing difficulty breathing
- The patient experiences worsening breathlessness
This mechanical restriction is a key reason why orthopnea develops and why patients instinctively avoid lying flat.
3. Increased Work of Breathing and Respiratory Muscle Fatigue
When lying flat:
- The respiratory system must work harder to maintain adequate ventilation
- Accessory muscles are recruited more heavily
- The diaphragm becomes less efficient
Over time, this leads to:
- Increased oxygen demand by respiratory muscles
- Fatigue of breathing muscles
- Sensation of trouble breathing or acute respiratory distress
Patients may describe this as:
- “I cannot breathe when I lie down”
- “I need extra pillows to breathe comfortably”
4. Ventilation–Perfusion (V/Q) Mismatch
Orthopnea is also associated with impaired gas exchange due to:
- Fluid accumulation in alveoli (especially in pulmonary edema)
- Collapse of dependent lung regions
- Poor oxygen diffusion across alveolar membranes
This results in:
- Reduced oxygenation
- Increased shortness of breath
- Worsening respiratory distress, especially during sleep
5. Role of Underlying Conditions
Orthopnea is commonly linked to:
- Heart failure or chronic kidney disease
- Fluid overload leads to pulmonary congestion
- Pulmonary edema
- Direct fluid accumulation in alveoli
- COPD
- Airflow limitation and air trapping worsen in supine position
- Acute respiratory distress syndrome (ARDS)
- Severe inflammation reduces lung compliance
In all these conditions, lying flat worsens respiratory mechanics, while sitting upright improves breathing.
How the Orthopneic Position Improves Respiratory Mechanics
The Orthopneic Position directly counteracts the physiological mechanisms that cause orthopnea. It is typically achieved by sitting upright at the edge of the bed, or in a chair, while leaning forward and resting on a support such as an overbed table, pillow, or knees for support.
1. Improved Lung Expansion
When a patient assumes the Orthopneic Position:
- The abdominal contents move downward due to gravity
- The diaphragm descends more freely
- The thoracic cavity expands more effectively
This leads to:
- Increased lung volume
- Better air entry and exit
- Reduced sensation of shortness of breath
Patients often report that this position helps them breathe better almost immediately.
2. Reduced Diaphragmatic Workload
Leaning forward in the Orthopneic Position:
- Optimizes diaphragmatic length–tension relationship
- Reduces mechanical compression of the diaphragm
- Allows more efficient contraction during inspiration
This reduces:
- Fatigue of respiratory muscles
- Sensation of difficulty breathing
3. Activation of Accessory Muscles
The position allows stabilization of the upper body using:
- Arms on an overbed table
- Arms on knees
- Support from pillows
This:
- Fixes the shoulder girdle
- Allows accessory muscles (sternocleidomastoid, scalene muscles) to assist breathing more effectively
- Reduces energy expenditure during respiration
4. Improved Heart–Lung Interaction
In patients with heart failure or chronic kidney disease:
- Upright positioning reduces venous return
- Decreases pulmonary congestion
- Improves oxygenation by reducing fluid overload in the lungs
This helps relieve:
- Breathlessness
- Respiratory distress
- Nocturnal symptoms such as paroxysmal nocturnal dyspnea
5. Enhanced Ventilation Efficiency
The Orthopneic Position improves:
- Ventilation-perfusion matching
- Alveolar recruitment in dependent lung regions
- Oxygen diffusion efficiency
This is especially important in:
- Pulmonary edema
- COPD exacerbations
- Acute respiratory distress
Clinical Example
A patient with heart failure or chronic kidney disease presents with worsening shortness of breath when lying flat. When placed in the Orthopneic Position—sitting upright on the side of the bed, leaning forward with arms resting on an overbed table—the patient experiences:
- Immediate relief of breathlessness
- Improved chest expansion
- Reduced respiratory rate
- Better oxygen saturation levels
This demonstrates how positioning alone can significantly improve respiratory mechanics without pharmacological intervention.
Conditions That Cause Orthopnea and Indicate Use of the Orthopneic Position
Orthopnea is a clinically significant symptom characterized by shortness of breath when lying flat, which is typically relieved by sitting upright in the Orthopneic Position. It is not a disease itself but a manifestation of underlying cardiac, pulmonary, or systemic conditions that impair normal respiratory and cardiovascular function. Understanding the conditions that cause orthopnea is essential for identifying patients who require immediate patient positioning to improve breathing and prevent worsening respiratory distress.
1. Cardiovascular Conditions
Heart Failure or Chronic Kidney Disease
One of the most common causes of orthopnea is heart failure or chronic kidney disease, where the heart is unable to efficiently pump blood, leading to fluid buildup in the lungs.
Pathophysiology includes:
- Increased venous return from the legs when lying flat
- Accumulation of extra blood in pulmonary circulation
- Increased hydrostatic pressure causing pulmonary congestion
This results in:
- Severe shortness of breath
- Reduced lung expansion
- Increased work of the heart and lungs
Patients often report needing to sit or stand to breathe comfortably and may sleep on top of several pillows or assume the Orthopneic Position to relieve shortness of breath.
Clinical Example
A patient with chronic heart failure may wake up at night experiencing paroxysmal nocturnal dyspnea, describing sudden trouble breathing that is only relieved when sitting upright in a supported position.
2. Pulmonary Conditions
Chronic Obstructive Pulmonary Disease (COPD)
In COPD (chronic obstructive pulmonary disease), airflow limitation and air trapping worsen when the patient lies flat. This leads to:
- Increased breathing difficulties
- Reduced expiratory efficiency
- Hyperinflation of the lung
Patients often assume a forward-leaning posture to improve ventilation, demonstrating that the Orthopneic Position helps reduce the work of breathing.
Pulmonary Edema
In pulmonary edema, fluid accumulates in the alveoli, impairing gas exchange. This causes:
- Severe dyspnea
- Hypoxia
- Frothy sputum in acute cases
The Orthopneic Position is used because it helps:
- Reduce pulmonary congestion
- Improve oxygenation
- Make breathing easier by reducing fluid pressure in the lungs
Acute Respiratory Conditions
In conditions such as acute respiratory distress syndrome (ARDS):
- Lung compliance is reduced
- Oxygen exchange is severely impaired
- Patients experience extreme acute respiratory distress
These patients often instinctively assume a sitting, forward-leaning posture to maximize ventilation.
3. Other Contributing Conditions
Fluid Overload States
Any condition causing fluid buildup, such as renal failure or excessive IV fluid administration, can lead to orthopnea. Increased circulating volume worsens pulmonary congestion when lying flat.
Obesity and Abdominal Pressure
Increased abdominal mass can:
- Push against the diaphragm
- Reduce maximum chest expansion
- Worsen shortness of breath when lying flat
Recognizing When a Patient Needs the Orthopneic Position
Early recognition of patients requiring the Orthopneic Position is critical in preventing deterioration of respiratory status. Nurses and clinicians must assess both subjective symptoms and objective clinical signs.
1. Key Symptoms Reported by the Patient
Patients who require the Orthopneic Position often report:
- Shortness of breath when lying flat
- Need to sleep with multiple pillows
- Feeling of breathlessness at night
- Relief of symptoms when sitting upright
- Episodes of trouble breathing that worsen in the recumbent position
A classic phrase often used is:
“I cannot breathe unless I sit up.”
2. Observable Clinical Signs
A patient who needs the Orthopneic Position may present with:
- Use of accessory muscles for breathing
- Rapid or labored respiratory rate
- Nasal flaring or visible respiratory distress
- Sitting at the edge of the bed leaning forward
- Resting arms on a pillow or overbed table for support
These behaviors indicate that the body is attempting to compensate for impaired lung function.
3. Behavioral and Postural Indicators
Patients instinctively adopt compensatory positions such as:
- Sitting upright in bed rather than lying down
- Leaning forward with arms supported on knees or furniture
- Avoiding the recumbent position due to worsening symptoms
- Preferring a position in bed that maximizes chest expansion
This spontaneous adaptation is a key clinical indicator of the need for the Orthopneic Position.
4. Clinical Decision-Making Indicators
Healthcare providers should initiate the Orthopneic Position when:
- Oxygen saturation drops in supine position
- Patient exhibits increasing breathing difficulties
- Signs of acute respiratory distress are present
- There is known history of heart failure or chronic kidney disease, COPD, or pulmonary edema
- Patient expresses inability to tolerate lying flat
Clinical Example
A patient with COPD admitted for exacerbation becomes increasingly short of breath when lying in bed. They are observed sitting at the side of the bed, leaning forward with arms supported on their knees. Oxygen saturation improves when placed in the Orthopneic Position, confirming its effectiveness in reducing respiratory distress and improving ventilation.
Nursing Patient Positioning Techniques in the Orthopneic Position
Effective patient positioning in the Orthopneic Position is a fundamental nursing intervention used to improve breathing, reduce respiratory distress, and support patients experiencing shortness of breath, breathlessness, or difficulty breathing. Proper technique is essential because incorrect positioning may worsen discomfort, increase fatigue of the diaphragm, or fail to optimize lung expansion.
The Orthopneic Position is typically achieved by positioning the patient in a sitting position, often at the edge of the bed, with the upper body inclined forward to maximize chest expansion and reduce the workload of the respiratory system.
1. Preparing the Environment for Positioning
Before assisting the patient, the nurse should ensure:
- The head of the bed is adjustable and can be elevated safely
- An overbed table or stable support surface is available
- Necessary pillows or supports are within reach
- Oxygen therapy equipment is ready if prescribed
- The environment is safe to reduce the risk of falling
This preparation ensures that the patient can assume the Orthopneic Position safely and comfortably, especially if they are experiencing acute breathing difficulties.
2. Step-by-Step Positioning Technique
The following steps outline safe and effective placement of a patient in the Orthopneic Position:
- Assist the patient into a sitting position
- Help the patient move from a recumbent position to sitting upright.
- Ensure the patient is stable at the edge of the bed if tolerated.
- Encourage forward leaning posture
- Instruct the patient to lean forward slightly.
- This forward flexion reduces pressure on the lungs and diaphragm.
- Provide upper body support
- Position an overbed table in front of the patient.
- Alternatively, place a pillow on the table for comfort.
- The patient may also rest arms on knees for support.
- Support arm placement
- Encourage the patient to rest arms on your knees or table.
- This creates a tripod-like base that helps stabilize the upper body.
- Adjust head and trunk alignment
- Ensure the head is aligned with the spine.
- Avoid excessive flexion that may restrict airway patency.
3. Position Variations for Comfort and Clinical Needs
Depending on the patient’s condition, variations may include:
- Semi-upright sitting with multiple pillows
- Fully upright sitting in a chair
- Edge-of-bed positioning with forward lean
- Use of additional pillows for chest or arm support
These variations help accommodate patients with varying levels of shortness of breath, acute respiratory distress, or fatigue.
4. Clinical Example
A patient with heart failure or chronic kidney disease experiencing fluid overload may be unable to lie flat due to severe breathlessness. The nurse assists the patient into a sitting position at the edge of the bed, places an overbed table in front, and supports the patient’s arms on a pillow. Within minutes, the patient reports reduced difficulty breathing and improved comfort.
Monitoring and Safety During Patient Positioning
Continuous monitoring and safety precautions are essential when maintaining a patient in the Orthopneic Position, especially in those with acute respiratory distress, COPD, or pulmonary edema.
1. Respiratory Monitoring
Nurses should closely observe:
- Respiratory rate and depth
- Signs of breathing difficulties or labored breathing
- Use of accessory muscles
- Presence of breathlessness or inability to speak in full sentences
- Oxygen saturation levels if monitored
Any worsening signs may indicate escalating respiratory distress requiring immediate intervention.
2. Cardiovascular Monitoring
Because the position affects venous return and cardiac workload, monitor:
- Heart rate and rhythm
- Signs of hypotension or dizziness
- Symptoms of fatigue or weakness
This is especially important in patients with heart failure or chronic kidney disease, where changes in positioning can significantly affect hemodynamics.
3. Safety Considerations
Key safety measures include:
- Preventing risk of falling, especially when the patient is sitting at the edge of the bed
- Ensuring stable support surfaces such as a locked overbed table
- Keeping call bell within reach
- Avoiding sudden position changes that may worsen shortness of breath
- Assisting patients who are weak or fatigued
4. Patient Comfort and Tolerance
The nurse should continuously assess:
- Patient ability to tolerate the position
- Degree of relief of shortness of breath
- Signs of fatigue or discomfort
- Need for repositioning or additional support
If the Orthopneic Position no longer relieves symptoms, escalation of care may be required.
5. Clinical Example of Monitoring
A patient with COPD placed in the Orthopneic Position shows initial improvement in breathing. However, after several minutes, oxygen saturation begins to drop and respiratory rate increases. The nurse recognizes worsening acute respiratory distress, re-evaluates the patient, and initiates oxygen therapy while notifying the healthcare provider.
Clinical Effectiveness and Limitations of the Orthopneic Position
The Orthopneic Position is widely recognized in clinical practice as a non-pharmacological intervention used to relieve shortness of breath, improve lung expansion, and reduce respiratory distress in patients experiencing conditions such as orthopnea, COPD (chronic obstructive pulmonary disease), and heart failure or chronic kidney disease. While its clinical benefits are well established through physiological principles and observational evidence, it is also important to understand its limitations in order to apply it appropriately within broader patient positioning strategies.
1. Clinical Effectiveness of the Orthopneic Position
1.1 Immediate Relief of Shortness of Breath
One of the most significant clinical benefits of the Orthopneic Position is its ability to rapidly relieve shortness of breath. Patients who experience difficulty breathing when lying flat often report immediate improvement when transitioning into a supported sitting position, particularly when leaning forward with support from a pillow, knees, or an overbed table.
This relief occurs because:
- The diaphragm moves more freely
- The lungs expand more effectively
- The work of breathing is reduced
Clinical Example
A patient with heart failure or chronic kidney disease experiencing pulmonary congestion may be unable to tolerate a recumbent position. When assisted into the Orthopneic Position at the edge of the bed, they often report reduced breathlessness within minutes due to improved ventilation and decreased venous congestion.
1.2 Improved Lung Expansion and Oxygenation
The Orthopneic Position significantly enhances lung expansion, particularly in patients with restrictive or obstructive pulmonary conditions. By reducing abdominal pressure on the diaphragm, the position allows for:
- Increased tidal volume
- Better alveolar ventilation
- Improved oxygen exchange
This is particularly beneficial in:
- COPD (chronic obstructive pulmonary disease)
- Pulmonary edema
- Acute respiratory distress syndrome (ARDS)
In these conditions, improved ventilation helps reduce breathing difficulties and enhances overall oxygen delivery to tissues.
1.3 Reduced Work of Breathing
Patients in respiratory distress often rely heavily on accessory muscles, leading to fatigue. The Orthopneic Position helps:
- Stabilize the upper body using a prop (table or knees)
- Reduce energy expenditure during breathing
- Improve efficiency of the respiratory system
This makes it especially useful during episodes of acute respiratory distress, where conserving energy is critical.
1.4 Cardiopulmonary Load Reduction
In patients with heart failure or chronic kidney disease, sitting upright reduces venous return and pulmonary congestion. This leads to:
- Decreased fluid accumulation in the lungs
- Reduced strain on the heart and lungs
- Improved breathing comfort
This mechanism explains why many patients instinctively sleep with multiple pillows or in a supported upright posture.
2. Limitations of the Orthopneic Position
Despite its benefits, the Orthopneic Position has important limitations that must be considered in clinical decision-making.
2.1 Not a Definitive Treatment
The Orthopneic Position is a supportive intervention, not a cure. It does not address the underlying causes of:
- Pulmonary edema
- COPD exacerbations
- Heart failure or chronic kidney disease
While it improves symptoms, it must be combined with:
- Oxygen therapy
- Medications (e.g., diuretics, bronchodilators)
- Definitive medical management
2.2 Limited Effect in Severe Respiratory Failure
In cases of severe acute respiratory distress syndrome (ARDS) or advanced respiratory failure:
- Positioning alone may not significantly improve oxygenation
- Patients may require mechanical ventilation or advanced respiratory support
In such cases, the Orthopneic Position is only an adjunctive measure.
2.3 Patient Fatigue and Tolerance Issues
Maintaining the Orthopneic Position for prolonged periods may cause:
- Fatigue in upper limb muscles
- Discomfort in the neck or back
- Reduced tolerance in elderly or critically ill patients
Some patients may require frequent repositioning or additional pillows for support.
2.4 Risk of Instability and Falling
When patients sit at the edge of the bed, there is an increased risk of falling, especially if they are:
- Weak
- Hypoxic
- Experiencing dizziness from acute respiratory distress
This requires close supervision during patient positioning.
2.5 Ineffectiveness in Non-Respiratory Causes of Dyspnea
Not all causes of shortness of breath respond to positioning. For example:
- Severe anemia
- Metabolic acidosis
- Neuromuscular respiratory failure
In these cases, the Orthopneic Position may provide minimal relief.
Evidence-Based Considerations in Respiratory Positioning
Evidence-based nursing practice supports the use of positioning strategies, including the Orthopneic Position, as part of a broader respiratory care plan. Research in respiratory physiology consistently shows that upright and forward-leaning positions:
- Improve lung expansion
- Enhance diaphragmatic efficiency
- Reduce work of breathing
- Improve oxygen saturation in patients with COPD and heart failure
However, evidence also emphasizes that positioning should be:
- Individualized based on patient condition
- Continuously reassessed for effectiveness
- Integrated with pharmacological and oxygen-based interventions
3.1 Clinical Assessment and Ongoing Evaluation
Nurses must evaluate whether the Orthopneic Position continues to:
- Reduce breathlessness
- Improve oxygenation
- Stabilize respiratory distress
If no improvement is observed, escalation of care is necessary.
Clinical Example (Evidence Application)
A patient with COPD (chronic obstructive pulmonary disease) admitted with severe breathing difficulties is placed in the Orthopneic Position using an overbed table for support. Initially, oxygen saturation improves and respiratory effort decreases. However, after progression of the disease, the position becomes less effective, indicating the need for bronchodilator therapy and possible ventilatory support.
Not confident in your nursing writing skills?
We’ll produce clear, professional, and evidence-based work.
Conclusion
The Orthopneic Position remains a fundamental and highly practical intervention in respiratory nursing care, particularly for patients experiencing orthopnea, shortness of breath, and varying degrees of respiratory distress. Its clinical value lies in its ability to immediately improve breathing comfort through simple yet effective patient positioning, typically achieved by supporting the patient in a sitting position and encouraging a forward lean using pillows, an overbed table, or knee support.
Across a wide range of conditions—including COPD (chronic obstructive pulmonary disease), pulmonary edema, heart failure or chronic kidney disease, and other causes of acute respiratory distress—the Orthopneic Position consistently demonstrates its ability to enhance lung expansion, reduce diaphragmatic workload, and improve overall efficiency of the respiratory system. In many cases, it serves as an early and visible indicator of disease severity, as patients instinctively adopt this posture when experiencing significant breathing difficulties.
However, while the position is highly effective in providing symptomatic relief, it is important to recognize that it does not treat the underlying pathology causing difficulty breathing. Instead, it functions as a supportive, non-pharmacological intervention that should be integrated into a broader clinical management plan, including oxygen therapy, medication, and ongoing assessment.
From a nursing perspective, the Orthopneic Position also reinforces the importance of careful observation, timely intervention, and individualized care. Recognizing when a patient assumes the Orthopneic Position, understanding what it signifies, and responding appropriately can significantly influence patient outcomes, comfort, and safety.
Ultimately, effective use of the Orthopneic Position reflects a core principle of nursing practice: that simple, well-executed interventions grounded in physiological understanding can make a profound difference in patient breathing, comfort, and overall clinical stability.
Frequently Asked Questions
What does orthopneic position do?
The orthopneic position improves breathing by allowing better lung expansion, reducing pressure on the diaphragm, and decreasing the work of breathing. It helps relieve shortness of breath, especially in patients who experience worsening symptoms when lying flat.
What position is best for dyspnea?
The best position for dyspnea (difficulty breathing) is usually an upright sitting position, such as the Orthopneic Position or tripod position, where the patient leans forward with support from pillows, a table, or knees. This position helps improve ventilation and reduces respiratory effort.
What is the orthopneic position for heart failure?
In heart failure, the orthopneic position involves sitting the patient upright—often at the edge of the bed—with support from an overbed table or pillows, while leaning forward. This helps reduce fluid congestion in the lungs, decreases venous return, and improves breathing.
What is the orthopneic position used for in surgery?
In surgical care, the orthopneic position is mainly used postoperatively or during respiratory distress management, not during surgery itself. It helps patients recover from anesthesia-related respiratory depression by improving lung expansion, enhancing oxygenation, and easing breathing difficulties during recovery.