
Positioning in the Operating Room: Complete Guide to the Lithotomy Position for Nursing Students
The lithotomy position is a fundamental patient position utilized extensively in both surgical and obstetric settings. Its application is critical for accessing the pelvic region, facilitating procedures in urological, gynecological, and pelvic surgeries, and assisting with childbirth during the second stage of labor. Proper patient positioning in lithotomy requires a comprehensive understanding of anatomical alignment, ergonomic principles, and potential risks to the lower extremities.
Clinical Relevance of the Lithotomy Position
- Surgical Access: The lithotomy position provides optimal exposure of the pelvic, perineal, and lower abdominal regions, allowing medical staff to perform procedures efficiently. Surgical procedures performed in the lithotomy position include:
- Gynecological surgeries such as hysterectomy, laparoscopy, and pelvic reconstructive surgeries.
- Urological procedures including cystoscopy, prostatectomy, and bladder repair.
- Other pelvic interventions requiring access to the perineum or lower abdomen.
- Obstetric Applications: During childbirth, the lithotomy position is often used in the second stage of labor to:
- Enhance visualization of the birth canal and perineum.
- Facilitate controlled delivery and management of perineal integrity.
- Allow the use of birthing interventions when necessary, such as episiotomy or assisted deliveries.
Principles of Proper Patient Positioning in Lithotomy
Proper positioning in the lithotomy position involves multiple considerations to ensure both patient safety and procedural success:
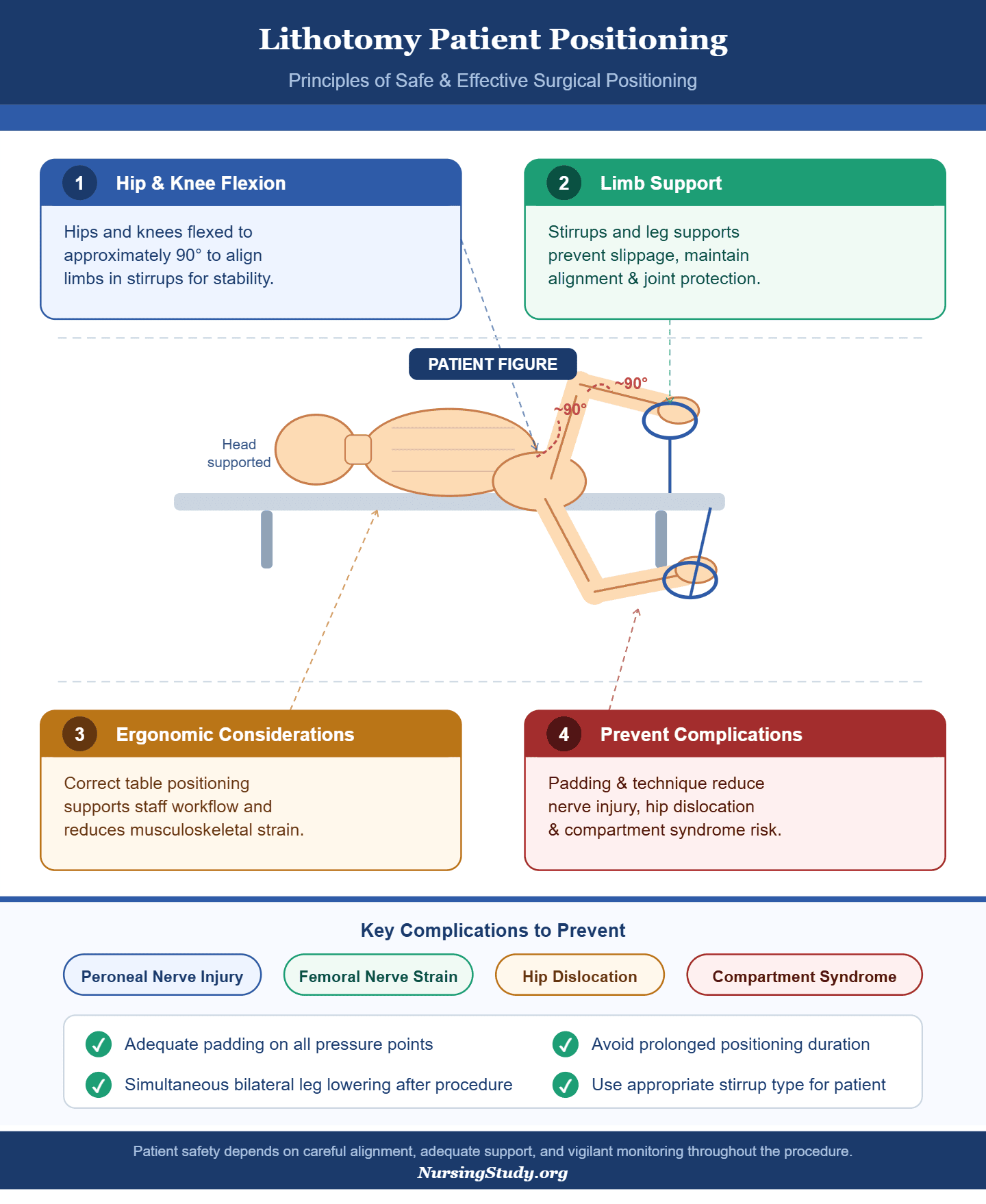
- Hip and Knee Flexion: The hips and knees are flexed, typically to approximately 90 degrees, to align the lower extremities in stirrups and maintain stability.
- Lower Extremities Support: Use of lithotomy stirrups or leg supports is essential to prevent slippage, maintain alignment, and minimize strain on joints and nerves.
- Ergonomic Considerations: Positioning the patient appropriately on the surgical table supports the staff’s workflow and reduces risk of musculoskeletal strain during prolonged procedures.
- Prevention of Complications: Proper padding and positioning techniques reduce the likelihood of peroneal nerve injury, femoral nerve strain, hip dislocation, and compartment syndrome.
Historical and Practical Context
The lithotomy position has its origins in both medical examinations and obstetric practice. Initially used to facilitate gynecological examinations and childbirth, it has evolved to become a standard position for many surgical procedures requiring access to the pelvic area. Its continued use in modern operating rooms demonstrates its effectiveness when proper positioning protocols are followed.
Proper Patient Positioning in the Lithotomy Position: Surgical and Birthing Applications
The lithotomy position is a cornerstone of patient positioning in both surgical procedures and obstetric care, designed to optimize access to the pelvic region while ensuring patient safety and comfort. Historically, this position evolved from early gynecological examinations and obstetric practices, where it was first used to facilitate exposure of the perineum and lower abdominal areas for examination and intervention. Over time, the position has been standardized to accommodate modern surgical techniques, birthing requirements, and ergonomic considerations for healthcare providers.
Clinical Relevance
In surgical settings, the lithotomy position is commonly used during gynecological procedures such as hysterectomy, pelvic reconstructive surgery, and laparoscopic interventions. Urological procedures including cystoscopy, prostatectomy, and bladder repair also rely on the patient being placed in the lithotomy position to provide unobstructed access to the pelvic organs. Beyond surgical applications, this position is essential during childbirth, particularly in the second stage of labor, as it facilitates controlled delivery and allows healthcare professionals to monitor the perineum and birth canal effectively.
Proper patient positioning in these contexts is critical because misalignment or inadequate support of the lower extremities can lead to complications such as peroneal nerve injury, femoral nerve strain, sciatic nerve injury, or compartment syndrome. These risks highlight the necessity of careful planning and adherence to positioning protocols.
Principles of Proper Patient Positioning
Proper positioning in the lithotomy position involves several key considerations:
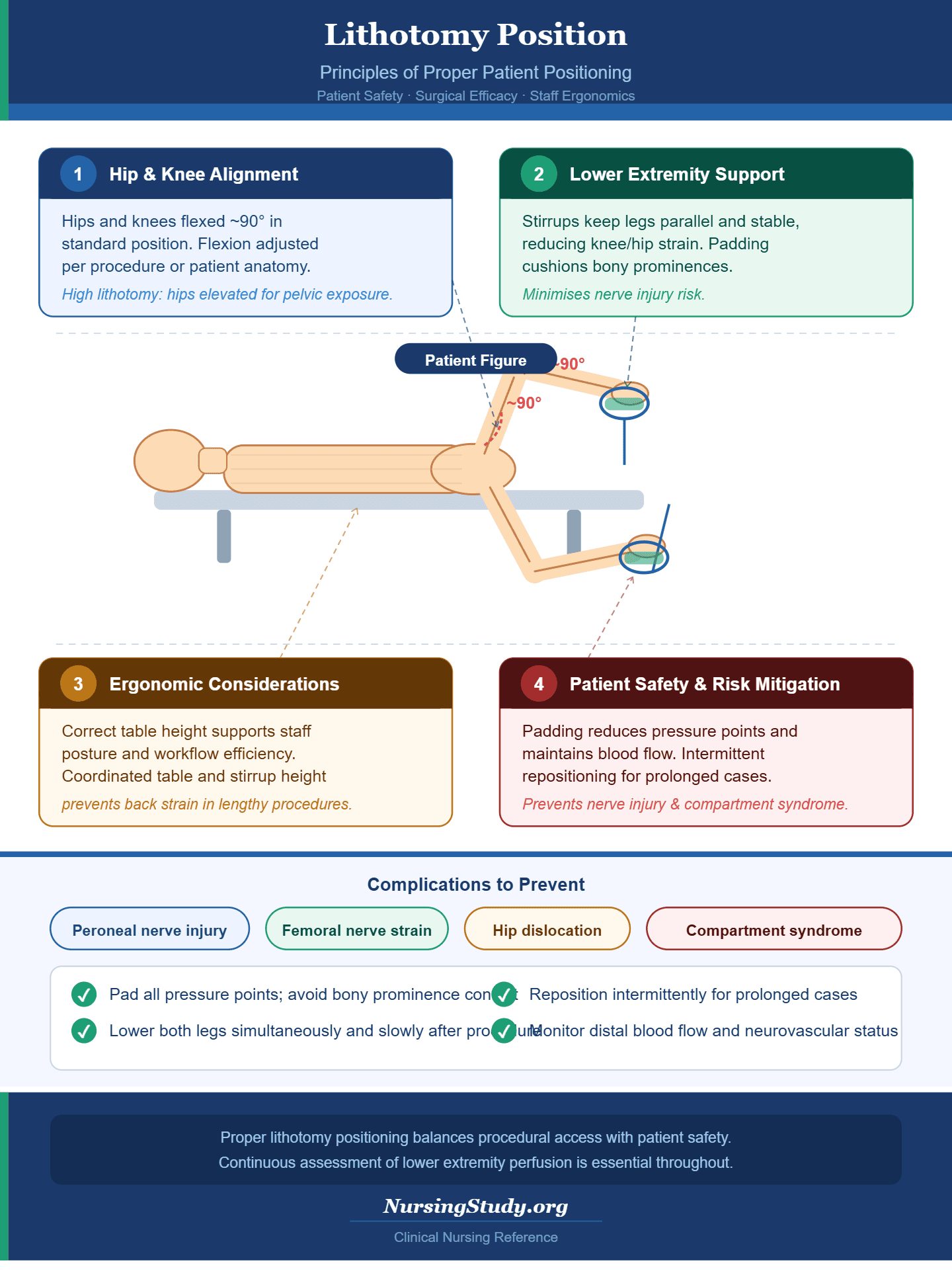
- Hip and Knee Alignment
- The hips and knees are flexed, often to approximately 90 degrees in the standard lithotomy position.
- The degree of flexion may be adjusted depending on the procedure, patient anatomy, or stage of labor.
- For example, during high lithotomy for certain gynecological surgeries, the hips may be elevated slightly above the level of the surgical table to provide better pelvic exposure.
- Lower Extremities Support
- Lithotomy stirrups are used to secure the patient’s legs, maintaining alignment and preventing slippage.
- Proper positioning of the stirrups ensures that the lower extremities are parallel and supported, reducing strain on the knees and hips and minimizing the risk of nerve injuries.
- Positioning pads may be added to cushion bony prominences and enhance comfort during prolonged procedures.
- Ergonomic Considerations for Medical Staff
- Correct patient placement allows surgeons and medical staff to work efficiently while maintaining ergonomically safe postures.
- For instance, raising or lowering the surgical table in coordination with lithotomy stirrups can prevent back strain or awkward movements during lengthy procedures.
- Patient Safety and Risk Mitigation
- Proper patient positioning involves ensuring the patient lies flat or slightly elevated on the operating table, with hips and knees supported, and legs securely in stirrups.
- Careful attention to the placement of lower extremities prevents compression of nerves, reduces pressure points, and maintains adequate blood flow to the lower legs.
- Patients undergoing prolonged lithotomy may require intermittent repositioning or adjustments to minimize the risk of complications associated with prolonged positioning, such as peroneal nerve injury or compartment syndrome.
Application in Surgical Procedures
When performing surgery in the lithotomy position, several procedural considerations are essential:
- Access to the surgical site: The position allows unobstructed visualization of the pelvic organs, perineum, and lower abdomen.
- Anesthesia considerations: The patient must be properly aligned to facilitate safe administration of general or regional anesthesia.
- Length of surgery: Longer procedures may require additional padding or periodic repositioning to protect the lower extremities.
For example, during a laparoscopic hysterectomy, the patient is placed in the lithotomy position with stirrups adjusted to elevate the legs and hips slightly, providing the surgeon with optimal access while maintaining patient safety.
Application in Childbirth
During childbirth, the lithotomy position supports controlled delivery and monitoring of the second stage of labor:
- Second Stage of Labor: The position enables obstetric staff to observe the perineum and facilitate the passage of the fetus through the birth canal.
- Birthing Position: Compared to alternative birthing positions such as lateral or squatting, the lithotomy position allows better access for interventions such as assisted delivery or episiotomy.
- Use of Lithotomy Stirrups: The stirrups provide stable support for the mother’s lower extremities, allowing for adequate flexion of the hips and knees while maintaining safety and comfort.
Confused about formatting or citations?
We’ll ensure your nursing assignment meets academic standards.
Understanding the Lithotomy Position
The lithotomy position is a widely used patient position in medical and surgical practice, designed to provide optimal access to the pelvic region while ensuring patient safety and procedural efficiency. Understanding its variations, anatomical considerations, and indications is essential for preventing complications and achieving successful outcomes.
Standard Lithotomy and Dorsal Lithotomy Variations
1. Standard Lithotomy Position
The standard lithotomy position is characterized by the patient lying on the back (supine position) on the surgical table with hips and knees flexed at approximately 90 degrees. The lower extremities are placed in lithotomy stirrups or leg supports, ensuring proper alignment and stability. Key features include:
- Hip Flexion: The hips are flexed to provide access to the pelvic region while maintaining patient comfort and safety.
- Knee Flexion: Knees are bent and supported by the stirrups, reducing strain on the lower leg and preventing hyperextension.
- Lower Extremities Alignment: Legs are positioned symmetrically, parallel, and securely in stirrups to minimize nerve compression and maintain circulation.
- Stirrup Adjustment: Lithotomy stirrups can be adjusted for height, angle, and lateral positioning to accommodate patient anatomy, procedural requirements, or stage of labor.
2. Dorsal Lithotomy Position
The dorsal lithotomy is a variation of the standard position, commonly used in gynecological and obstetric procedures. In this position, the patient is supine with the pelvis slightly elevated, often using a tilt of the operating table or additional padding. Differences compared to the standard lithotomy include:
- Increased Hip Flexion: Hips may be flexed beyond 90 degrees to allow enhanced access to the pelvic cavity.
- Enhanced Pelvic Tilt: Elevation of the pelvis improves visualization during pelvic surgery or childbirth.
- Leg Support Considerations: Additional supports or straps may be used to stabilize the lower extremities and prevent slippage.
The choice between standard and dorsal lithotomy depends on procedural requirements, patient anatomy, and anticipated duration of surgery or childbirth. Proper understanding of these variations is critical to avoid complications associated with lithotomy, such as peroneal nerve injury or compression-related vascular compromise.
Indications: When and Why the Lithotomy Position is Used
1. Surgical Procedures
The lithotomy position is commonly used in a wide range of surgical procedures, particularly those involving the pelvic region. These include:
- Gynecological Procedures: Hysterectomy, pelvic reconstructive surgery, laparoscopic ovarian procedures, and colposcopy.
- Urological Procedures: Cystoscopy, prostatectomy, bladder repairs, and urethral surgeries.
- Pelvic Surgeries: Rectal surgeries, pelvic floor repairs, and certain hernia procedures.
The position provides unobstructed access to the surgical site, improves visualization, and allows medical staff to perform procedures efficiently while maintaining patient safety. For example, in a laparoscopic hysterectomy, the lithotomy position allows the surgeon to manipulate instruments in the pelvic cavity without obstruction from the lower extremities.
2. Obstetric Applications
During childbirth, the lithotomy position is commonly employed in the second stage of labor to facilitate controlled delivery. Key applications include:
- Access to the Birth Canal: The position allows healthcare providers to monitor fetal descent and assist with delivery interventions if necessary.
- Perineal Visualization: Proper patient positioning ensures clear visualization of the perineum, helping to minimize trauma during the second stage of labor.
- Controlled Delivery: When episiotomy or assisted delivery is required, the lithotomy position enables optimal leg positioning using stirrups, providing stability and access.
3. Rationale for Choosing the Lithotomy Position
The lithotomy position is selected over alternative birthing or surgical positions for several reasons:
- Enhanced Access and Exposure: Compared to lateral or prone positions, lithotomy provides superior exposure of the pelvic region and perineum.
- Ease of Interventions: In surgical procedures, lithotomy facilitates manipulation of instruments and access to the surgical site. In childbirth, it enables controlled maneuvers to assist fetal delivery.
- Patient Safety and Ergonomics: When properly executed, the lithotomy position minimizes risk to the patient’s lower extremities and allows medical staff to work efficiently without compromising posture or workflow.
4. Example of Clinical Application
A patient undergoing a urological procedure, such as cystoscopy, is placed in the lithotomy position with hips and knees flexed at 90 degrees, legs secured in lithotomy stirrups, and the pelvis slightly elevated. This alignment allows the surgeon to access the bladder efficiently while maintaining lower leg circulation and minimizing the risk of peroneal or femoral nerve injury. Similarly, during the second stage of labor, the mother’s lower extremities are supported in stirrups to enable controlled delivery while reducing strain on the knees and hips.
Placing a Patient in Lithotomy: Step-by-Step Guide
Proper patient positioning in the lithotomy position requires meticulous planning and execution, whether for surgical procedures or childbirth. Correct placement ensures patient safety, maintains blood flow to the lower extremities, and optimizes access to the surgical or birthing site.
Preparing the Operating Room and Patient
1. Operating Table Adjustment
- Begin by adjusting the surgical table to an appropriate height and tilt to facilitate safe placement of the patient. For most procedures, the table should allow the patient to be supine with slight elevation of the pelvis if necessary.
- Ensure the table is stable and can accommodate lithotomy stirrups while maintaining sterility. Certain procedures may require Trendelenburg position to improve pelvic exposure, but the table tilt should always balance access with patient safety.
2. Maintaining Sterility
- All areas of the table and stirrups that may come into contact with the patient’s lower extremities should be draped with sterile covers when the procedure requires sterile access.
- Medical staff must wear sterile gloves when adjusting lithotomy stirrups after the patient is positioned to avoid contamination.
3. Pre-Procedure Assessment and Positioning Checklist
Before placing the patient in lithotomy:
- Assess for risk factors associated with nerve injuries, hip dislocation, or compartment syndrome.
- Evaluate patient mobility, hip and knee flexibility, and existing musculoskeletal or vascular conditions.
- Ensure padding for bony prominences to reduce compression injuries.
- Confirm patient comfort and understanding of the positioning process.
- A checklist may include: verifying stirrup adjustment, table stability, padding placement, and alignment of the lower extremities.
Adjusting Lithotomy Stirrups and Lower Extremities
1. Stepwise Placement in Lithotomy
- Begin with the patient supine on the operating table.
- Gently flex the hips and knees, typically to 80–90 degrees in standard lithotomy, or more in high lithotomy for surgical access.
- Position each leg into the lithotomy stirrups carefully, ensuring alignment of the lower extremities.
- Adjust stirrup height and angle to maintain symmetry and prevent excessive abduction or adduction.
2. Securing the Lower Extremities
- Ensure legs are parallel and supported, with knees and calves resting comfortably in the stirrups.
- Check that straps or stirrup supports do not compress the peroneal nerve or femoral nerve, which could lead to nerve injuries.
- Positioning pads or foam supports can be placed under heels, calves, or knees to prevent slippage and reduce pressure points.
3. Maintaining Circulation and Safety
- Avoid extreme hip flexion or prolonged prolonged lithotomy position that can compromise blood flow.
- Periodically reassess lower extremities during lengthy procedures to detect early signs of nerve compression or ischemia.
- Ensure proper patient positioning in lithotomy minimizes risk of sciatic nerve injury and compartment syndrome.
Considerations for the Second Stage of Labor
1. Patient Management During Childbirth
- In the second stage of labor, the lithotomy position during childbirth provides controlled access to the birth canal and perineum.
- The mother’s hips and knees are flexed and supported in lithotomy stirrups, which allows obstetric staff to monitor fetal descent and guide delivery effectively.
2. Effects on the Perineum and Delivery
- Proper alignment and support of the lower extremities reduce excessive stretching or tearing of the perineum.
- Compared to alternative birthing positions such as lateral or squatting, lithotomy facilitates interventions like episiotomy, assisted delivery, or forceps application.
3. Balancing Comfort and Procedural Needs
- Adequate padding and adjustment of stirrups enhance comfort while preventing nerve compression.
- During delivery, periodic repositioning or slight adjustments may be necessary to maintain maternal comfort and fetal safety.
- Staff should remain vigilant for signs of prolonged pressure or nerve injuries associated with lithotomy.
4. Example of Clinical Application
During a vaginal delivery, the patient is placed in lithotomy with hips flexed at 90 degrees, knees supported in stirrups, and the pelvis slightly elevated. This positioning allows the obstetric team to guide fetal descent, observe perineal changes, and perform controlled interventions without compromising blood flow to the lower extremities or increasing the risk of peroneal or femoral nerve injury.
Complications and Risks Associated with the Lithotomy Position
While the lithotomy position is widely used in surgery and childbirth due to its accessibility and procedural benefits, it is associated with specific risks and complications that must be understood to ensure safe patient care. Proper awareness, preventive strategies, and monitoring are crucial to mitigate these risks.
Nerve Injuries and Lower Extremity Risks
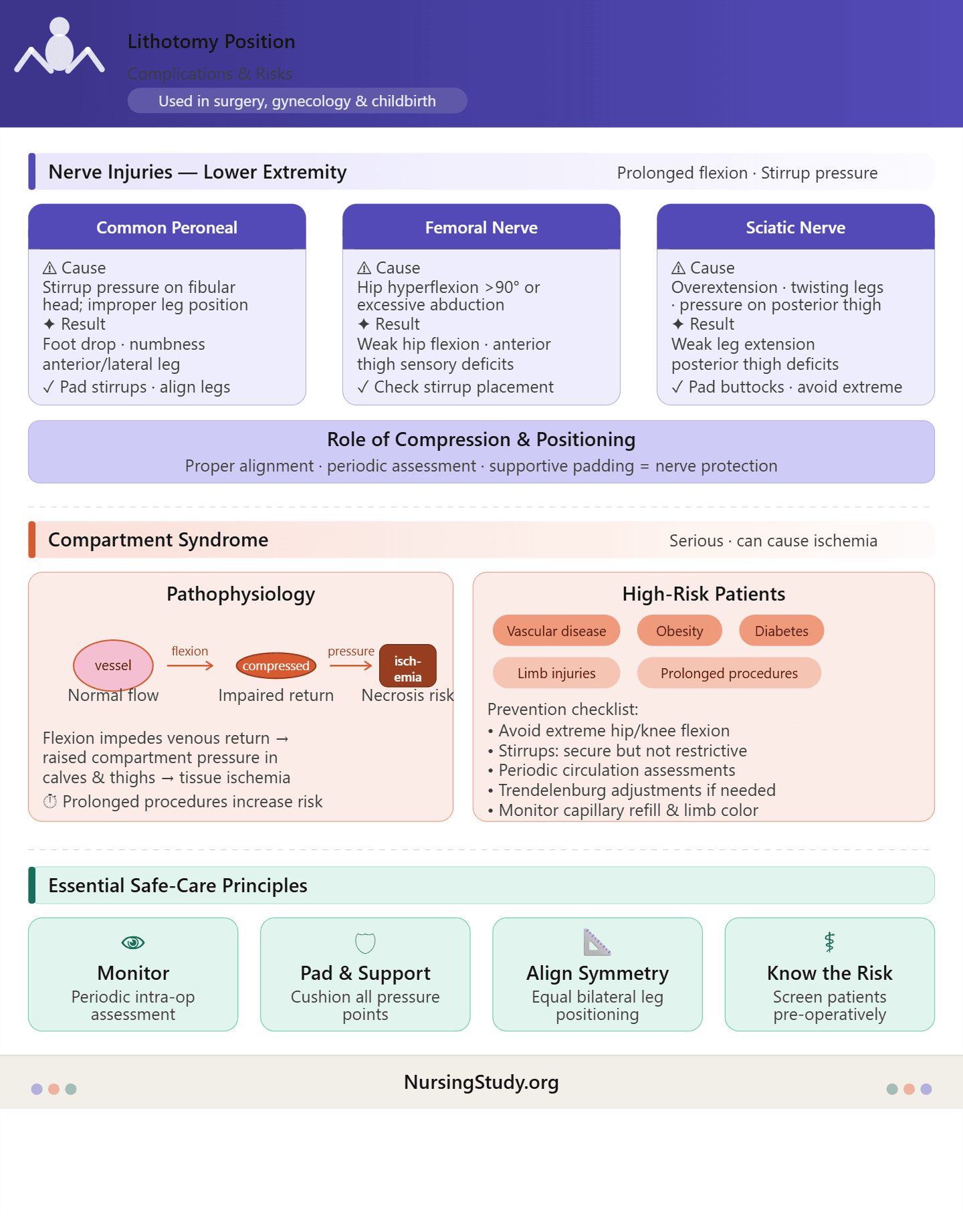
The lithotomy position can predispose patients to nerve injuries due to prolonged flexion, improper leg support, or excessive pressure on the lower extremities. The most commonly affected nerves include the peroneal nerve, femoral nerve, and sciatic nerve.
1. Common Peroneal Nerve Injury
- Cause: Compression against the lateral aspect of the fibular head by stirrups or improper positioning of the lower leg.
- Manifestation: Foot drop, numbness, or tingling along the anterior and lateral aspects of the lower leg and dorsum of the foot.
- Prevention: Ensure that lithotomy stirrups are padded, legs are aligned symmetrically, and knees are not abducted excessively. Avoid prolonged compression in prolonged lithotomy position.
2. Femoral Nerve Injury
- Cause: Hyperflexion of the hips beyond 90 degrees or excessive abduction can stretch or compress the femoral nerve.
- Manifestation: Weakness in hip flexion, difficulty extending the knee, and anterior thigh sensory deficits.
- Prevention: Maintain appropriate hip and knee flexion and check stirrup placement to avoid undue stretch.
3. Sciatic Nerve Injury
- Cause: Overextension or twisting of the legs, improper padding under the buttocks, or prolonged pressure on the posterior thigh.
- Manifestation: Weakness in leg extension, difficulty walking, and sensory deficits along the posterior thigh and lower leg.
- Prevention: Use proper positioning pads, avoid extreme abduction, and ensure the lower legs are parallel in the stirrups.
Role of Compression and Positioning
Compression and sustained flexion in the operating room contribute significantly to nerve injuries associated with lithotomy. Proper alignment, periodic assessment during surgery, and use of supportive padding are essential for nerve protection.
Risk Factors for Compartment Syndrome
Compartment syndrome is a serious complication that can arise from prolonged pressure or impaired circulation in the lower extremities during lithotomy procedures.
1. Patients at Risk
- Individuals with pre-existing vascular disease, obesity, diabetes, or lower limb injuries.
- Prolonged surgical procedures or extended prolonged lithotomy position.
- Patients with tight stirrup placement or excessive flexion of hips and knees.
2. Pathophysiology
- Flexion of the lower extremities in stirrups can impede venous return and increase compartment pressures in the calves and thighs.
- Reduced perfusion may result in ischemia and tissue necrosis if not recognized early.
3. Prevention
- Avoid extreme hip and knee flexion beyond recommended angles.
- Ensure lithotomy stirrups provide secure but not restrictive support.
- Periodically assess circulation, capillary refill, and limb color during lengthy procedures.
- In high-risk patients, consider Trendelenburg position adjustments or lateral positioning to improve perfusion.
Obstetric Considerations
During childbirth, the lithotomy position facilitates access to the birth canal and perineum but introduces specific obstetric risks:
1. Perineal Trauma
- Cause: Prolonged lithotomy positioning with hips and knees flexed may increase tension on the perineum.
- Manifestation: Increased incidence of perineal tears, episiotomy complications, or tissue edema.
- Prevention: Gentle controlled delivery, proper birthing position, and padding under the lower extremities.
2. Effects on the Second Stage of Labor
- Lithotomy positioning may affect fetal descent and maternal pushing mechanics, potentially lengthening the second stage of labor if not managed carefully.
- Controlled flexion of hips and knees and proper leg support ensures optimized delivery mechanics and minimizes trauma.
3. Clinical Example
- During a vaginal delivery, a mother placed in lithotomy with lithotomy stirrups and lower extremities adequately padded allows for direct observation of the perineum, controlled episiotomy if needed, and rapid intervention to assist fetal delivery. Misalignment or excessive flexion, however, could increase risk factors associated with nerve injury or perineal trauma.
Best Practices for Safe Lithotomy Positioning
Proper execution of the lithotomy position is critical to patient safety during surgical procedures and childbirth. While this position provides excellent access to the pelvic and perineal regions, incorrect or prolonged positioning can result in serious complications, including nerve injuries, compartment syndrome, and lower extremity ischemia. Adhering to best practices ensures both procedural efficiency and patient safety.
Preventing Complications in Surgery and Childbirth
1. Proper Patient Positioning
- Alignment of Hips and Knees: Flex the hips and knees to appropriate angles—commonly 80–90 degrees in standard lithotomy. Avoid hyperflexion or excessive abduction, which can increase the risk of femoral nerve or sciatic nerve injury.
- Lower Extremities Placement: Keep the lower legs parallel and aligned in lithotomy stirrups. Ensure the legs are secure but not tightly compressed to maintain blood flow to the lower extremities.
- Padding and Positioning Pads: Use soft padding under knees, calves, and heels to prevent compression injuries to the common peroneal nerve. This also reduces pressure on bony prominences, which is especially important in prolonged lithotomy position.
2. Stirrup Safety
- Height and Angle Adjustment: Adjust the lithotomy stirrups to match patient anatomy, ensuring symmetry between both legs. High or uneven stirrups increase the risk of hip dislocation or nerve stretch injuries.
- Securing the Legs: Use padded stirrup supports or straps carefully. Legs must be snugly supported but must allow micro-movements to prevent venous stasis.
- Avoiding Compression: Never let straps compress the lateral knee region or calf, which could cause peroneal nerve injury or reduce perfusion to the lower leg.
3. Procedure-Specific Considerations
- During gynecological, urological, or pelvic surgery, proper lithotomy positioning improves access to the surgical site while minimizing risk to nerves and soft tissues.
- In childbirth, particularly during the second stage, maintaining appropriate hip and knee angles facilitates controlled delivery, reduces perineal trauma, and supports safe use of lithotomy stirrups.
- Use positioning in the operating room protocols to verify proper patient setup prior to incision or delivery.
Monitoring and Adjustments
1. Periodic Checks During Surgery or Childbirth
- Lower Extremities Assessment: Every 30–60 minutes during prolonged procedures, inspect the lower extremities for color, temperature, swelling, or signs of ischemia.
- Nerve Monitoring: Check for any tingling, numbness, or unusual positioning that could indicate sciatic, peroneal, or femoral nerve stress.
- Hip and Knee Angles: Reassess the flexion of hips and knees periodically to ensure the patient remains in a safe position in surgery.
2. Integration into Operating Room Protocols
- Hospitals and surgical centers should have standardized protocols for positioning in the operating room. This includes checklists for proper patient positioning, stirrup adjustment, padding placement, and periodic reassessment.
- Use of a positioning pad checklist ensures all critical steps are followed, preventing complications associated with prolonged lithotomy.
- Team communication is key; nurses, surgical techs, and anesthesiologists should confirm patient is placed correctly before and during procedures.
3. Documentation and Post-Procedure Evaluation
- Document the patient in lithotomy details, including hip and knee angles, stirrup type, padding placement, and any adjustments made during the procedure.
- Postoperative assessment should include evaluation for nerve function, perineal integrity, and signs of compartment syndrome. Early recognition of complications allows for prompt intervention, reducing long-term morbidity.
4. Example of Clinical Application
- During a 3-hour pelvic surgery, the patient is placed in standard lithotomy with hips and knees flexed at 90 degrees. Foam pads are positioned under the knees and calves, and stirrup height is adjusted symmetrically. Every 45 minutes, the surgical team verifies leg alignment, skin color, and perfusion. This approach minimizes risk of peroneal nerve injury, sciatic nerve injury, and lower leg ischemia, while providing optimal surgical access.
Alternatives and Special Considerations
While the lithotomy position is a common position in both surgical and obstetric procedures, it is not universally appropriate. Certain clinical scenarios, patient conditions, or surgical requirements necessitate deviation from lithotomy to ensure safety and optimize outcomes. Understanding alternative positions and special considerations is crucial for safe positioning in the operating room.
When to Use Trendelenburg or Lateral Positions Instead
1. Trendelenburg Position
The Trendelenburg position involves tilting the operating table so that the patient’s head is lower than the pelvis. This position is occasionally used as an alternative or adjunct to lithotomy position for specific surgical or obstetric indications.
- Clinical Situations:
- To improve exposure during pelvic surgery when the surgeon requires enhanced access to the lower abdomen without excessive flexion of hips and knees.
- In cases of hypotension, the Trendelenburg position can improve venous return to maintain perfusion.
- During childbirth, it may be used temporarily to reposition the patient in lithotomy when fetal descent requires gravity-assisted maneuvers.
- Comparison with Lithotomy:
- Unlike the standard lithotomy, the Trendelenburg position reduces extreme hip flexion, potentially lowering risk factors associated with nerve injuries.
- However, Trendelenburg does not allow the same level of access to the perineum or pelvic surgical site, limiting its use for procedures requiring direct visualization, such as gynecological or urological lithotomy procedures.
2. Lateral Position
The lateral position involves placing the patient on their side with lower extremities slightly flexed or supported. It is used in both surgical and obstetric care when lithotomy position is contraindicated.
- Clinical Situations:
- Patients with hip dislocations, severe obesity, or lower leg injuries that prevent safe flexion of hips and knees.
- Surgeries where perineal access is not required, or the surgeon requires alternative exposure to the pelvic or abdominal region.
- Obstetric cases where prolonged lithotomy may increase peroneal nerve injury risk or perineal trauma.
- Comparison with Lithotomy:
- Lateral positioning avoids extreme flexion of hips and knees, reducing compression on the peroneal, femoral, or sciatic nerves.
- However, lateral positioning may limit access to the birth canal and is not ideal for direct perineal assessment during second stage of labor.
Adaptations for High-Risk Patients
Certain patients require modifications to the lithotomy position due to pre-existing conditions. These adaptations help prevent complications while maintaining surgical or birthing access.
1. Patients with Lower Extremity Injuries
- Avoid excessive hip and knee flexion.
- Use adjustable lithotomy stirrups with additional padding.
- Align the lower extremities symmetrically to minimize risk of sciatic nerve injury or compartment syndrome.
2. Obese Patients
- Use reinforced or high lithotomy stirrups capable of supporting increased weight without compressing lower legs.
- Maintain proper alignment of hips and knees to avoid hip dislocation or excessive compression of femoral and peroneal nerves.
- Consider intermittent lowering of the legs if prolonged lithotomy is anticipated to preserve perfusion and prevent nerve injuries.
3. Patients with Vascular Disease
- Avoid extreme abduction and flexion of hips and knees, which could compromise circulation.
- Utilize padding and positioning pads to support lower extremities and prevent ischemia.
- Monitor lower leg perfusion closely during surgery or childbirth, adjusting stirrups or operating table tilt as needed.
4. Special Obstetric Considerations
- For patients at higher risk of perineal trauma or with previous pelvic surgeries, slight modification of lithotomy position during childbirth may involve lowering hips and knees slightly or using birthing positions with reduced abduction.
- Controlled adjustments facilitate safer passage through the birth canal, minimizing trauma during the second stage of labor.
5. Example of Clinical Adaptation
- In a 70-year-old patient with peripheral vascular disease scheduled for pelvic surgery, the patient is placed in a modified lithotomy position with hips flexed to 70 degrees and knees to 80 degrees. Padded lithotomy stirrups are used, and the operating table is slightly tilted to improve venous return. Frequent assessment of the lower extremities ensures perfusion and minimizes risk factors associated with compartment syndrome and nerve injuries.
Confused about formatting or citations?
We’ll ensure your nursing assignment meets academic standards.
Conclusion
The lithotomy position remains one of the most pivotal patient positions in both surgical procedures and childbirth, offering unparalleled access to the pelvic and perineal regions. Its widespread use in gynecological, urological, and pelvic surgeries, as well as during the second stage of labor, underscores its clinical significance. However, the position is not without risks. Improper flexion of the hips and knees, misalignment of lower extremities, or incorrect use of lithotomy stirrups can lead to serious complications, including peroneal, femoral, and sciatic nerve injuries, compartment syndrome, and perineal trauma.
Effective positioning in the operating room hinges on understanding both the mechanics of the lithotomy position and the unique needs of each patient. Best practices emphasize careful adjustment of lithotomy stirrups, use of positioning pads, and vigilant monitoring of lower extremities during procedures. Modifications for high-risk patients—such as those with obesity, lower extremity injuries, or vascular compromise—further enhance safety while maintaining surgical or birthing access. Alternative positions, including the Trendelenburg or lateral positions, provide viable options when traditional lithotomy positioning is contraindicated, ensuring that care remains patient-centered and evidence-based.
From a clinical perspective, the success of procedures in lithotomy position depends on collaboration among medical staff, adherence to proper patient positioning protocols, and ongoing assessment throughout the duration of the procedure or labor. By integrating ergonomic principles, positioning checklists, and patient-specific adaptations, healthcare providers can minimize risks, optimize outcomes, and promote the safety and comfort of patients in both surgical and obstetric settings.
In essence, mastery of the lithotomy position is not solely about placing a patient on the operating table; it is about balancing access to the surgical site or birth canal with neurological protection, vascular perfusion, and perineal integrity. When executed with precision, attention to detail, and adherence to evidence-based practices, the lithotomy position becomes a safe and effective tool that supports both procedural efficiency and patient-centered care.
Frequently Asked Questions
What is a lithotomy position used for?
The lithotomy position is used to provide optimal access to the pelvic and perineal regions during surgical procedures, including gynecological, urological, and pelvic surgeries, as well as during childbirth, particularly in the second stage of labor. It facilitates patient in lithotomy access for procedures while supporting lower extremities with lithotomy stirrups.
What are the 4 types of position?
The four basic types of patient position commonly used in clinical care are:
- Supine position – patient lies flat on the back.
- Prone position – patient lies flat on the abdomen.
- Lateral position – patient lies on the side, used for high-risk patients or specific procedures.
- Lithotomy position – patient lies on the back with hips and knees flexed, legs supported in lithotomy stirrups for access to the pelvic region.
What are the 8 positions used in nursing?
The eight patient positions frequently applied in nursing include:
- Supine position
- Prone position
- Lateral position
- Sims’ position – semi-prone, for rectal exams or enema administration.
- Fowler’s position – semi-upright, for respiratory comfort or feeding.
- High Fowler’s position – upright at 90 degrees, often used during second stage of labor.
- Trendelenburg position – head-down tilt for surgical exposure or hypotension management.
- Lithotomy position – used for pelvic surgeries and birthing procedures, with lower extremities supported.
Why is lithotomy position used for delivery?
The lithotomy position during childbirth is used to provide direct access to the birth canal and perineum, facilitating controlled delivery, obstetric interventions, and use of instruments if necessary. It allows medical staff to monitor the fetal descent during the second stage of labor, supports proper patient positioning, and enables efficient perineal management, though alternatives like upright or lateral birthing positions may reduce perineal trauma in some cases.