
Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy (TAH BSO): Surgical Procedure, Oophorectomy, and Patient Care for Nursing Students
Total Abdominal Hysterectomy (TAH) and Bilateral Salpingo-Oophorectomy (TAH-BSO) is a major gynecologic surgical procedure that combines the removal of the uterus and cervix with the removal of both ovaries and fallopian tubes. This surgical procedure is commonly performed for a range of benign and malignant conditions affecting the female reproductive system, allowing direct access to the pelvis and surrounding structures through an abdominal incision.
The procedure is indicated when conservative treatments fail or are inappropriate. Benign indications include symptomatic uterine fibroids, endometriosis, persistent abnormal uterine bleeding, or chronic pelvic pain. Malignant indications encompass ovarian cancer, endometrial cancer, and occasionally cervical cancer, where removal of the uterus, cervix, ovaries and fallopian tubes, and sometimes lymph nodes is necessary for staging and management of the disease. In such cases, TAH-BSO can be performed alongside a radical hysterectomy to ensure complete tumor excision and reduce the risk of recurrence.
TAH-BSO significantly alters female reproductive and endocrine anatomy. Removal of the ovaries induces surgical menopause, which may lead to hot flashes, vaginal dryness, and other hormonal changes. Decisions regarding hormone replacement therapy should be individualized based on patient age, comorbidities, and cancer risk. The procedure also requires careful intraoperative management to protect adjacent structures such as the ureter, bowel, and vagina.
From a surgical perspective, TAH-BSO involves a meticulous dissection of the uterus and cervix, ligation of supporting ligaments, and excision of the fallopian tubes and ovaries through an abdominal incision. Compared to vaginal or laparoscopic hysterectomy, the abdominal approach provides direct visualization of the pelvis, which is essential when addressing tumors, cysts, or extensive endometriosis. Proper perioperative care, including general anesthesia, infection prevention, and postoperative monitoring, is crucial to minimize risks and side effects, such as blood clots, wound complications, or injury to the rectum and other pelvic structures.
The purpose of this discussion is to provide a thorough overview of TAH-BSO, including its indications, detailed surgical steps, potential complications, and postoperative considerations. Understanding the anatomy, surgical technique, and physiological impact of this procedure is essential for safe and effective management, optimizing patient outcomes, and supporting recovery.
Understanding Hysterectomy, Total Abdominal Hysterectomy, and Bilateral Salpingo-Oophorectomy (tahbso) in Gynecologic Care
Hysterectomy and Total Abdominal Hysterectomy: Anatomy, Indications, and Surgical Procedure
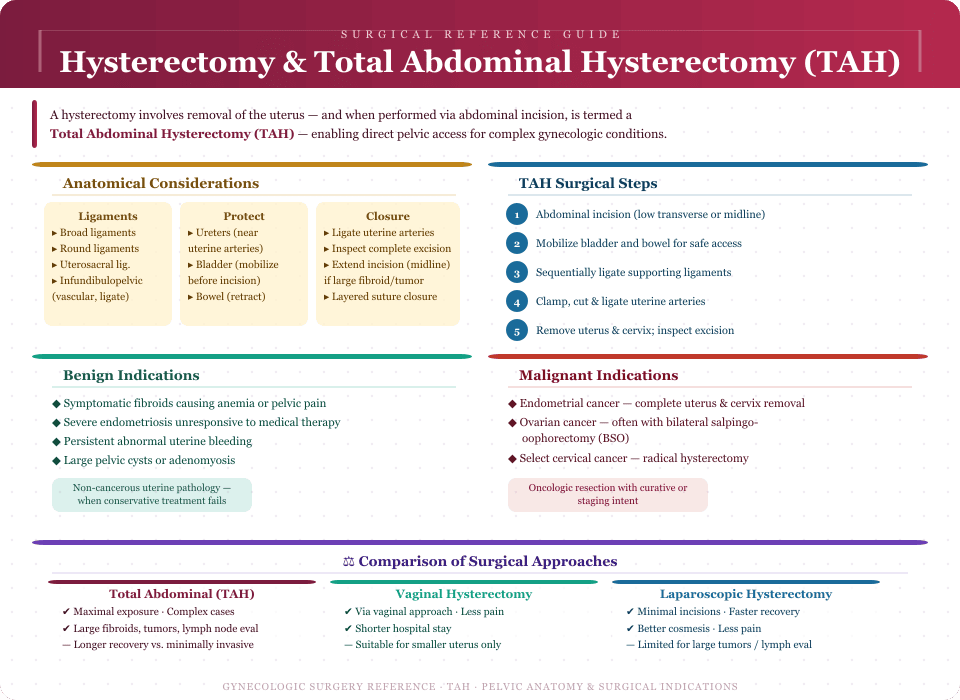
A hysterectomy is a surgical procedure involving the removal of the uterus, and depending on the procedure, may also involve removal of the cervix, fallopian tubes, and ovaries. When performed via a low transverse or midline abdominal incision, the procedure is called a total abdominal hysterectomy (TAH). This approach provides direct access to the pelvis, allowing for careful management of complex gynecologic conditions such as large fibroids, extensive endometriosis, cysts, or malignant tumors of the uterus and cervix.
Anatomical Considerations
Understanding the pelvic anatomy is critical for safe TAH. The uterus is supported by multiple ligaments, including the broad ligaments, round ligaments, and uterosacral ligaments, which maintain uterine position within the pelvis. The fallopian tubes and ovaries are connected to the uterus via the infundibulopelvic ligament, containing vascular structures that must be carefully ligated to prevent hemorrhage. The ureters run close to the uterine arteries and must be protected during ligation, while the bowel and bladder are mobilized to prevent inadvertent injury.
During TAH, the uterus and cervix are mobilized by sequentially ligating these ligaments. The uterine arteries are clamped, cut, and ligated, minimizing intraoperative bleeding. In cases of large fibroids or tumors, the abdominal wall may be extended via a midline incision to improve exposure. Once removed, the uterus is inspected for complete excision, and the abdominal incision is closed using layered sutures, ensuring integrity of the pelvis and abdominal wall.
Indications
TAH is indicated for both benign and malignant conditions.
- Benign indications:
- Symptomatic fibroids causing anemia or pelvic pain
- Severe endometriosis unresponsive to medical therapy
- Persistent abnormal uterine bleeding
- Large pelvic cysts or adenomyosis
- Malignant indications:
- Endometrial cancer requiring complete removal of the uterus and cervix
- Ovarian cancer, often performed in conjunction with bilateral salpingo-oophorectomy
- Select cases of cervical cancer, where a radical hysterectomy may be necessary
Comparison with Other Approaches
While TAH provides maximal exposure, other approaches include:
- Vaginal hysterectomy: Performed through the vagina, offering reduced postoperative pain and a shorter hospital stay. Suitable for smaller uterine sizes without extensive pelvic pathology.
- Laparoscopic hysterectomy: Includes total laparoscopic or laparoscopic-assisted vaginal hysterectomy, utilizing small abdominal incisions for improved cosmesis, faster full recovery, and less pain. Limited for large fibroids, tumors, or when lymph nodes need evaluation.
Example: A 48-year-old woman with a 12-cm uterine fibroid causing anemia and recurrent pelvic pain may undergo TAH rather than laparoscopic hysterectomy, as direct access allows complete removal and safe control of the uterine arteries.
Bilateral Salpingo-Oophorectomy (BSO) and Oophorectomy: Procedure, Hormonal Impact, and TAH-BSO Considerations
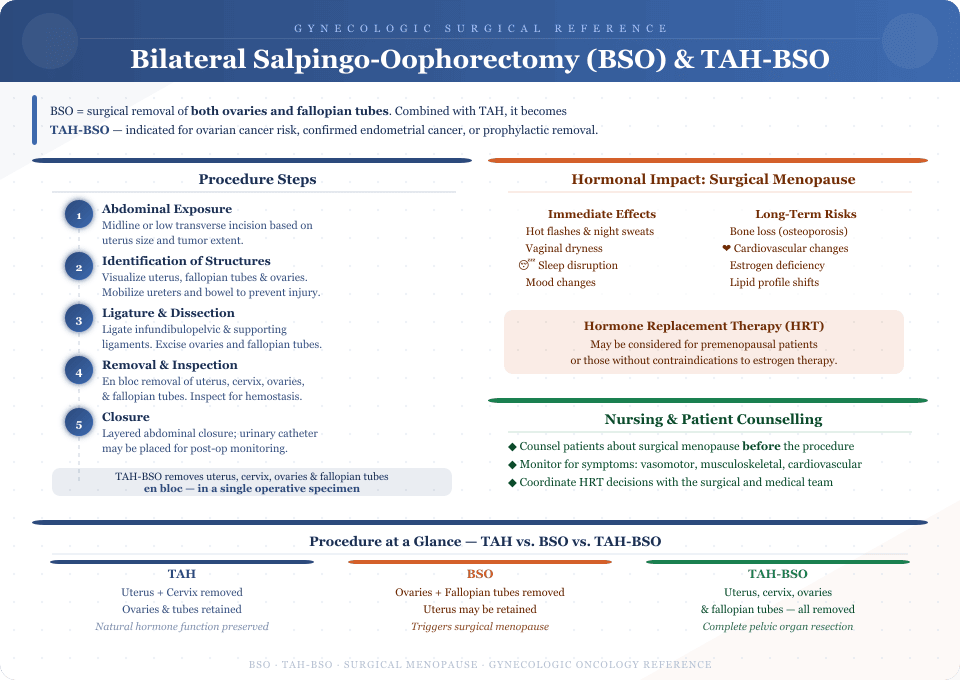
Bilateral salpingo-oophorectomy (BSO) is the surgical removal of both ovaries and fallopian tubes. When combined with TAH, it is termed TAH-BSO or total abdominal hysterectomy and bilateral salpingo-oophorectomy. This procedure is especially indicated in patients with high risk of ovarian cancer, confirmed endometrial cancer, or those requiring prophylactic removal of the ovaries and fallopian tubes.
Procedure Steps
- Abdominal Exposure: The abdomen is opened via a midline or low transverse incision, depending on the size of the uterus and tumor.
- Identification of Structures: The uterus, fallopian tubes, and ovaries are carefully visualized. The ureters and bowel are mobilized to avoid injury.
- Ligature and Dissection: The infundibulopelvic ligament and supporting ligaments are ligated to control blood flow. The ovaries and fallopian tubes are excised.
- Removal and Inspection: If performing TAH-BSO, the uterus, cervix, ovaries, and fallopian tubes are removed en bloc. The pelvic cavity is inspected for hemostasis and tumor spread.
- Closure: The abdominal incision is closed in layers, and a catheter may be left temporarily for urinary monitoring.
Hormonal Impact
Removal of the ovaries leads to surgical menopause, which may cause hot flashes, vaginal dryness, and long-term risks such as bone loss and cardiovascular changes. Hormone replacement therapy may be considered in premenopausal patients or those without contraindications. Nurses and healthcare providers must counsel patients about these effects and monitor for symptom management.
Example: A 52-year-old patient with a BRCA mutation may undergo TAH-BSO to reduce her lifetime risk of ovarian cancer and simultaneously manage an early-stage endometrial cancer. Postoperatively, she may require hormone replacement therapy and counseling on vaginal dryness and hot flashes.
Indications for Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy (TAH BSO) in Endometrial and Ovarian Cancer
TAH-BSO is indicated for both benign and malignant conditions.
- Benign: Symptomatic fibroids, severe endometriosis, recurrent cysts, or pelvic pain.
- Malignant: Endometrial cancer, ovarian cancer, and selective cases of cervical cancer.
Surgical Considerations
- Enables assessment of the pelvis, excision of tumors, and evaluation of lymph nodes for metastasis.
- When indicated, a radical hysterectomy may be performed to achieve wider excision margins for cervical or endometrial cancer.
- Prophylactic removal of the ovaries and fallopian tubes may reduce future risk of ovarian cancer or prevent recurrence of cysts.
Clinical Example: A 55-year-old woman diagnosed with early-stage ovarian cancer undergoes total abdominal hysterectomy with bilateral salpingo-oophorectomy with pelvic lymph node dissection to ensure complete excision and staging. Conversely, a 45-year-old with large fibroids causing anemia may undergo TAH-BSO to alleviate symptoms while lowering her risk of ovarian pathology in the future.
Surgical Procedure of Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy (TAH-BSO)
Preoperative Preparation, Anesthesia, and Patient Care in TAH BSO
Total Abdominal Hysterectomy (TAH) and Bilateral Salpingo-Oophorectomy is a major gynecologic surgical procedure requiring meticulous preoperative preparation. Before undergoing hysterectomy, a healthcare provider conducts a thorough evaluation to optimize patient care and reduce risks and side effects.
- Medical assessment: Comprehensive review of cardiac, pulmonary, and renal status to identify conditions that may increase the risk during abdominal surgery.
- Laboratory and imaging studies: Complete blood count, coagulation profile, and imaging such as ultrasound, CT, or MRI to evaluate the uterus, ovaries and fallopian tubes, fibroids, cysts, endometriosis, or tumor.
- Patient education and consent: Discussion of surgical removal of the uterus and cervix, removal of the ovaries, potential surgical menopause, hot flashes, vaginal dryness, and the role of hormone replacement therapy. Patients are informed about the time of hysterectomy, expected hospital stay, and full recovery.
- Bowel preparation: May be indicated to reduce risk of bowel injury, especially in cases involving extensive dissection.
General anesthesia is used for TAH-BSO, providing relaxation of the abdominal wall and pelvis for safe surgical technique. Nursing staff assist with positioning, monitor vital signs, manage the catheter, and ensure that bowel, ureters, and rectum are protected during the procedure.
Abdominal Incision and Total Abdominal Hysterectomy with Bilateral Removal of Uterus, Ovaries, and Fallopian Tubes
The surgical technique for TAH-BSO is carefully tailored to the patient’s condition:
- Incision: A low transverse abdominal incision is preferred for smaller uterus or fibroids, providing quicker full recovery. A midline abdominal incision is used for large tumors or extensive endometriosis.
- Exposure and Dissection: The uterus and cervix, ovaries and fallopian tubes, and pelvic structures are mobilized. The bowel and ureters are identified and protected throughout dissection.
- Ligature of Ligaments: The broad ligament (leaf of the broad ligament), uterosacral ligaments, and round ligaments are ligated to safely mobilize the uterus. Infundibulopelvic ligaments are dissected for removal of the ovaries.
- Removal of Uterus, Cervix, Ovaries, and Fallopian Tubes: The uterus and cervix are excised. In endometrial or cervical cancer, a radical hysterectomy may remove surrounding ligaments and a portion of the vagina to achieve clear surgical margins.
- Closure: The abdominal wall and incision are closed in layers with sutures, ensuring hemostasis and reducing risks and side effects.
Example: A patient with multiple fibroids and early-stage endometrial cancer undergoes TAH-BSO, allowing removal of the uterus and cervix, fallopian tubes and ovaries, and assessment of lymph nodes for staging.
Managing Tumor, Lymph Nodes, and Endometrial Cancer During TAH BSO
In patients with gynecologic cancer, including ovarian cancer and endometrial cancer, TAH-BSO allows for:
- Tumor Resection: Complete removal of uterus, cervix, ovaries, and fallopian tubes, including any visible tumor.
- Lymph Node Assessment: Pelvic lymph nodes are evaluated to identify potential spread.
- Radical Hysterectomy vs TAH: In cervical or advanced endometrial cancer, radical hysterectomy removes additional ligaments and upper vagina to ensure negative surgical margins.
Example: For early-stage ovarian cancer, TAH-BSO combined with lymph node sampling reduces risk for ovarian cancer recurrence while enabling accurate staging.
Postoperative Complications and Nursing Assessment After Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy
Postoperative care involves vigilant monitoring to promote full recovery and identify complications early. Nurses monitor vital signs, the abdominal incision, urine output via catheter, and bowel function to detect injury to the ureters or rectum.
Common Complications:
- Surgical menopause following removal of the ovaries, leading to hot flashes, vaginal dryness, and consideration of hormone replacement therapy.
- Infection at the abdominal incision or within the pelvis.
- Bleeding from ligated vessels or pelvic dissection sites.
- Blood clots in the legs or pelvis.
- Injury to bowel or ureters during surgical technique.
- Long-term pelvic changes, including pelvic organ prolapse or recurrence of cysts.
Patient Education: Patients are counseled on activity restrictions, wound care, monitoring for risks and side effects, and use of hormone replacement therapy after surgical menopause. Typically, patients stay in the hospital for a few days after abdominal surgery, with gradual return to normal activities over weeks after surgery.
Example: A patient with endometrial cancer undergoing TAH-BSO may experience vaginal dryness and hot flashes; ongoing support from the healthcare provider ensures safe recovery and adaptation to surgical menopause.
Nursing Care and Patient Management After TAH-BSO Surgery
Total Abdominal Hysterectomy (TAH) and Bilateral Salpingo-Oophorectomy (TAH-BSO) represents a significant gynecologic surgical procedure with both immediate and long-term implications for the patient’s health. Effective nursing care after this surgery is critical to promote full recovery, minimize complications, and support adaptation to changes such as surgical menopause and hormone replacement therapy.
Pain Management, Wound Care, and Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy Patient Care
Postoperative pain management is one of the primary concerns following abdominal hysterectomy with bilateral salpingo-oophorectomy. Pain is typically localized at the abdominal incision and may radiate to the pelvis due to uterus and cervix removal and dissection of surrounding ligaments and pelvic structures. Adequate pain control facilitates early mobilization, reduces the risk of blood clots, and supports respiratory function. Healthcare providers often use a combination of analgesics, including intravenous opioids in the immediate postoperative period, followed by oral medications as tolerated.
Wound care is equally essential to prevent infection at the abdominal wall. Nurses monitor for erythema, drainage, or dehiscence at the abdominal incision, ensuring that sutures remain intact and that proper hygiene is maintained. Patients are instructed on how to keep the incision clean and dry, and the timing of suture removal or dressing changes is coordinated according to the surgical technique used.
Catheter management is another critical aspect of postoperative care. A catheter is usually placed during TAH-BSO to monitor urine output and prevent bladder distention. Nursing staff assess for urinary retention, infection, or trauma to the ureter, and remove the catheter as soon as the patient can safely void independently. Early ambulation and mobilization are encouraged to enhance bowel motility, reduce blood clot formation, and prevent pelvic organ complications.
Patient Education on Activity, Vaginal Care, and Hormone Replacement Therapy After TAH-BSO
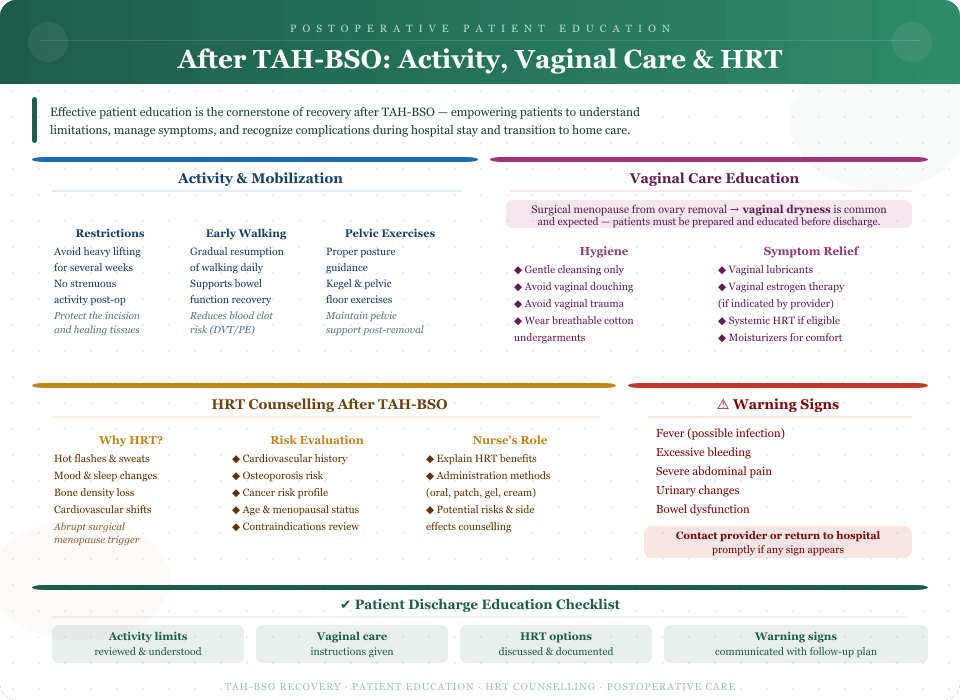
Patient education is a cornerstone of postoperative care following TAH-BSO. Effective instruction ensures that patients understand the limitations and expectations during the hospital stay and the transition to home care.
Activity and Mobilization:
- Patients are advised to avoid heavy lifting or strenuous activity for several weeks after surgery.
- Gradual resumption of walking supports bowel function and reduces the risk of blood clots.
- Proper posture and pelvic exercises may be recommended to maintain pelvic support after uterus removal.
Vaginal Care:
- Patients may experience vaginal dryness due to surgical menopause, especially when removal of the ovaries has occurred.
- Education includes gentle cleansing of the vagina, avoidance of vaginal trauma, and use of lubricants or vaginal estrogen therapy as indicated.
Hormone Replacement Therapy (HRT) Counseling:
- After TAH-BSO, abrupt surgical menopause may lead to hot flashes, mood changes, and bone density loss.
- Healthcare providers evaluate the patient’s individual risk for cardiovascular disease, osteoporosis, and cancer before initiating hormone replacement therapy.
- Nurses play a key role in explaining HRT benefits, administration methods, and potential risks and side effects.
Signs of Complications:
- Patients are taught to recognize early warning signs such as fever, excessive bleeding, abdominal pain, urinary changes, or bowel dysfunction.
- Clear instructions on when to contact the healthcare provider or return to the hospital ensure prompt management of complications.
Supporting Recovery and Long-Term Patient Care Following Total Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy
Recovery after TAH-BSO extends beyond the hospital stay. Comprehensive nursing care incorporates both physical and emotional health support.
Follow-Up and Monitoring:
- Regular follow-up appointments monitor abdominal incision healing, assess pelvic health, and evaluate adaptation to surgical menopause.
- Surveillance may include imaging or lab tests for patients with ovarian cancer or endometrial cancer to ensure no recurrence of tumor or cysts.
Lifestyle and Rehabilitation:
- Patients are encouraged to engage in low-impact exercise and maintain a healthy diet to support bone health and cardiovascular function, particularly after removal of the ovaries.
- Pelvic floor exercises may reduce the risk of pelvic organ prolapse and improve urinary and bowel function.
Emotional and Reproductive Health Support:
- Nurses provide counseling for emotional adjustment to surgical menopause, changes in sexual function, and the loss of fertility after TAH-BSO.
- Support groups and therapy may be recommended to address vaginal dryness, hot flashes, and psychological adaptation.
Example: A patient undergoing total abdominal hysterectomy with bilateral salpingo-oophorectomy for endometrial cancer receives guidance on incision care, pain management, gradual mobilization, and hormone replacement therapy. She attends follow-up visits for pelvic assessment, receives counseling on activity restrictions and vaginal care, and is provided with resources for managing surgical menopause and emotional wellbeing.
Clinical Scenarios and Case Studies for Nursing Students on TAH and BSO
TAH-BSO in Gynecologic Oncology: Ovarian Cancer, Endometrial Cancer, and Tumor Management
Total Abdominal Hysterectomy (TAH) and Bilateral Salpingo-Oophorectomy (TAH-BSO) is frequently indicated in gynecologic oncology for conditions such as ovarian cancer, endometrial cancer, and other pelvic tumors. In these cases, the procedure not only involves the removal of the uterus and cervix but also the ovaries and fallopian tubes to reduce the risk for ovarian cancer and manage malignant disease.
Scenario 1 – Ovarian Cancer:
A 52-year-old patient presents with a suspicious pelvic mass and elevated CA-125 levels. Imaging reveals a tumor involving the ovary and the fallopian tube. During TAH-BSO, the surgeon removes the uterus and cervix, fallopian tubes and ovaries, and performs pelvic lymph node assessment. The nursing staff monitors anesthesia effects, assists in dissection and protection of the bowel and ureters, and educates the patient preoperatively about the potential for surgical menopause and hormone replacement therapy. Postoperatively, nurses assess the abdominal incision, manage the catheter, and monitor for blood clots, infection, or bowel dysfunction.
Scenario 2 – Endometrial Cancer:
A 60-year-old patient with endometrial hyperplasia unresponsive to conservative therapy undergoes abdominal hysterectomy with bilateral salpingo-oophorectomy. The uterus and cervix, along with ovaries and fallopian tubes, are removed, and lymph nodes are sampled to evaluate tumor spread. The nursing staff plays a critical role in perioperative care, including monitoring for bleeding, assessing pelvic pain, and providing education about vaginal care and activity restrictions during the hospital stay.
These clinical scenarios illustrate that TAH-BSO in gynecologic oncology requires not only surgical precision but also careful nursing assessment and patient-centered management to optimize full recovery and long-term outcomes.
Nursing Assessments and Decision-Making During TAH-BSO Surgical Procedure
Effective nursing care during TAH-BSO combines clinical vigilance, patient safety, and anticipation of potential complications:
- Preoperative Assessment: Confirm patient history, laboratory results, imaging, and understanding of surgical technique; educate about incision care, catheter management, and hormone replacement therapy.
- Intraoperative Monitoring: Monitor general anesthesia, vital signs, and blood loss. Assist with dissection to protect bowel, ureters, and rectum. Ensure the uterus and cervix, ovaries, and fallopian tubes are removed completely when indicated.
- Decision-Making: Nurses must anticipate complications such as inadvertent ureteral injury, bowel perforation, or excessive bleeding, facilitating prompt intervention by the healthcare provider.
Example: If intraoperative findings reveal extensive endometriosis or a tumor infiltrating the pelvis, the nursing staff ensures additional instruments and sutures are available, monitors for extended anesthesia time, and prepares for potential radical hysterectomy.
Recognizing and Managing Postoperative Complications in Abdominal Hysterectomy with Bilateral Salpingo-Oophorectomy
Early detection of postoperative complications is crucial for patient safety and optimal recovery. Nurses monitor for:
- Bowel Complications: Constipation, ileus, or inadvertent rectal injury. Bowel sounds and function are assessed regularly, and early mobilization is encouraged.
- Urinary Complications: Monitor for urinary retention or ureteral obstruction, especially after removal of the uterus and ovaries. Catheter output and urinalysis are routinely checked.
- Wound and Pelvic Complications: Assess the abdominal incision for signs of infection, dehiscence, or hematoma. Monitor for pelvic pain or abnormal drainage.
Example: A patient post-TAH-BSO develops mild abdominal wall swelling and tenderness. The nurse identifies early infection at the abdominal incision, notifies the healthcare provider, and initiates wound care with antibiotics, preventing progression to a more serious complication.
Long-Term Patient Care Strategies for TAH-BSO Recovery
Long-term recovery after TAH-BSO focuses on both physical and emotional health:
- Monitoring for Surgical Menopause: Removal of the ovaries induces abrupt menopause, resulting in hot flashes, vaginal dryness, and possible bone density loss. Patients are counseled on hormone replacement therapy options.
- Pelvic Health and Rehabilitation: Pelvic floor exercises and proper activity restrictions reduce the risk of pelvic organ prolapse and support urinary and bowel function.
- Follow-Up and Surveillance: Patients with a history of ovarian cancer or endometrial cancer require regular imaging, lab tests, and pelvic exams to detect recurrence or new tumors.
- Emotional Support and Counseling: Nursing staff provides guidance on reproductive changes, coping with surgical menopause, and sexual health after TAH-BSO.
Example: A patient recovering from total abdominal hysterectomy with bilateral salpingo-oophorectomy for ovarian cancer attends follow-up appointments to monitor lymph nodes, manages hormone replacement therapy, and receives counseling on vaginal care and activity limitations while gradually returning to normal life.
Conclusion
Total Abdominal Hysterectomy (TAH) and Bilateral Salpingo-Oophorectomy (TAH-BSO) represents one of the most significant gynecologic surgical procedures, combining the removal of the uterus and cervix with oophorectomy and excision of the fallopian tubes. This procedure is critical in managing both benign conditions, such as fibroids and endometriosis, and malignant diseases, including ovarian cancer, endometrial cancer, and select cervical cancers. The decision to perform TAH-BSO is guided by comprehensive evaluation of tumor involvement, lymph nodes, pelvic anatomy, and patient-specific risk factors, emphasizing the importance of thorough preoperative assessment, imaging, and patient education.
From a nursing care perspective, TAH-BSO requires meticulous attention to perioperative and postoperative management. Nurses play a pivotal role in pain management, incision care, catheter monitoring, and early identification of bowel, ureteral, or pelvic complications. Long-term patient care focuses on managing surgical menopause, addressing hot flashes, vaginal dryness, and counseling on hormone replacement therapy. Supporting full recovery also involves activity guidance, pelvic rehabilitation, and ongoing surveillance for recurrence in gynecologic oncology cases.
Clinical scenarios underscore the complexity of TAH-BSO, demonstrating how nursing assessments, intraoperative decision-making, and postoperative vigilance contribute directly to patient safety and optimal outcomes. Whether addressing the removal of ovaries in a patient at high risk of ovarian cancer or managing the abdominal incision in patients recovering from extensive dissection of uterus and cervix, nurses are central to ensuring both physiological and emotional well-being.
Ultimately, understanding the surgical procedure, its indications, and the nuances of postoperative care allows healthcare providers to reduce risks and side effects, improve patient care, and enhance recovery trajectories. By integrating knowledge of TAH, bso, total abdominal hysterectomy with bilateral removal of tubes and ovaries, and associated long-term health considerations, clinicians and nurses alike can optimize outcomes and provide holistic care for patients undergoing this life-changing gynecological TAH-BSO procedure.
Frequently Asked Questions
What is a total abdominal hysterectomy with bilateral salpingo-oophorectomy procedure?
A total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO) is a gynecologic surgical procedure in which the uterus, cervix, both ovaries, and fallopian tubes are removed through an abdominal incision. This procedure is commonly performed for endometrial cancer, ovarian cancer, fibroids, endometriosis, or other significant gynecologic conditions. The surgery may involve careful dissection of pelvic structures and assessment of lymph nodes to reduce the risk of ovarian cancer or tumor spread.
Can a woman still get wet after a total hysterectomy?
Yes. Sexual arousal and vaginal lubrication are primarily controlled by hormonal and vascular factors. After a TAH-BSO, especially if the ovaries are removed, surgical menopause may lead to vaginal dryness. However, with proper hormone replacement therapy or the use of lubricants, many women can maintain normal vaginal function and sexual response.
What is one of the main indicators for a total abdominal hysterectomy with bilateral salpingo-oophorectomy?
One of the main indications for TAH-BSO is gynecologic cancer, such as endometrial cancer or ovarian cancer. Other indications include large or symptomatic fibroids, severe endometriosis, or a high risk of ovarian cancer that cannot be managed conservatively.
What is the difference between a hysterectomy and a TAH-BSO?
A hysterectomy refers generally to the surgical removal of the uterus, and may be partial (leaving the cervix) or total (removing the uterus and cervix). A TAH-BSO, or total abdominal hysterectomy with bilateral salpingo-oophorectomy, is more extensive—it includes removal of the uterus, cervix, both ovaries, and fallopian tubes. The TAH-BSO has additional hormonal and reproductive implications due to the removal of the ovaries, often resulting in surgical menopause.